Tracking and Preventing the Health Impacts of Extreme Heat
The response to the 9/11 terrorist attacks included building from scratch a bioterrorism-monitoring system that remains a model for public health systems worldwide. Today we face a similarly galvanizing moment: weather-related hazards cause multiple times the 9/11 death toll each year, with extreme heat often termed the “top weather killer,” at 1,670 official deaths a year and 10,000 attributed via excess deaths analysis. Extreme cold and dense wildfire smoke each cause comparable numbers of deaths. By rapidly upgrading and expanding the health-tracking systems of the Centers for Disease Control (CDC), Veterans Health Administration (VHA), and Centers for Medicare and Medicaid (CMS) to improve real-time surveillance of health impacts of climate change, the U.S. can similarly meet the current moment to promote climate-conscientious care that save lives.
Challenge and Opportunity
The official death toll of extreme heat since 1979 stands at over 11,000, but the methods used to develop this count are known to underestimate the true impacts of heat waves. The undercounting of deaths related to extreme heat and other people-centered disasters — like extreme cold and smoke waves — hinders the political and public drive to address the problem and adds difficulty to declaring heat waves as disasters despite the massive loss of life. Similarly, the lack of integration of critical environmental data like “wet bulb” temperature alongside these health impacts in electronic data systems hinders the provision of medical care.
National Accounting
The national reaction to the 9/11 terrorist attacks provides a roadmap forward: improved data and tracking is fundamental to a nation’s evidence-based threat response. Operated by federal, state, and local public health professionals who comprise the CDC’s National Syndromic Surveillance Program (NSSP), surveillance systems were developed across the nation to meet new challenges in disease detection and situational awareness. Since 2020, the CDC’s Data Modernization Initiative (DMI) has provided a framework for this transformation, with the stated goal of improving the nation’s ability to predict, understand, and share data on new health threats in real time. While the DMI has focused on the pioneering role of new technologies for health protection, this effort also offers a once-in-a-generation opportunity for the public health and medical surveillance establishment to increase their capacity to address pressing future threats to the nation’s welfare, including the evolving climate crisis. Increasingly, extreme weather is responsible for both near-term disasters (more frequent and intense heat waves, dense smoke waves, and cold waves) and the long-term exacerbation of prevalent health conditions (such as heart, lung, and neurological disease). Its increasingly severe impacts demand a detailed and funded roadmap to attain the DMI’s goals of “real-time, scalable emergency response” capability.
Patient Care
Syndromic surveillance systems track the impacts of events at a population level, but other resources are needed to directly help individual patients during a disaster. Electronic health records (EHRs) allow medical providers to track relevant information that could help diagnose arising health conditions. Some medical systems have begun tracking nonmedical information to assist in diagnosis, such as the social determinants of health (e.g., housing and food availability) that are linked to improving patient outcomes. However, the environmental conditions a patient has experienced are not typically linked to health records. Improving the links between environmental conditions and EHRs will help patients—for example, by determining if a new asthma diagnosis is related to recent smoke waves—and also support syndromic surveillance.
A similar effect occurs with death records. Death records are typically logged at the patient level with free-form text that is mostly up to a medical professional who is often under time pressure. Text for each death record is later coded to fit into specific cause codes as it is aggregated into population-level datasets such as the National Vital Statistics System. Information about the environmental conditions that contributed to the death can be lost at any step along the process, resulting in the undercount of climate-related mortality. Improved tracking at the individual level will improve accounting at the national level.
Plan of Action
In order to track the health impacts from extreme weather events and thereby enhance the provision of medical care during such events, both disaster and health data must be improved.
Recommendation 1. National accounting for health impacts of the climate crisis
The National Syndromic Surveillance Program provides a world-class starting point for better tracking of climate health impacts, both in terms of technology and a dedicated and knowledgeable workforce. The following plan will permit the evolution of this underlying infrastructure to provide health systems and policy makers with real-time and forecast impacts.
To modernize real-time monitoring of health impacts:
- CDC should actively support efforts within the NSSP to expand tracking of more conditions tied to the health impacts of extreme weather events. In parallel, new research initiatives are needed to link these new surveillance syndromes with health system burden and health outcomes to improve the real-world predictive utility of these efforts.
- CDC should work with the Department of Education to track school closures and student absences, and with OSHA to track work-related injuries during extreme weather conditions. The National Institute for Occupational Safety and Health (NIOSH) at CDC will be a key partner in developing worker tracking as they already conduct surveillance including worker absenteeism and mortality. Similar programs should be constructed for schools, for example, leveraging the student attendance counts already collected by states to make a school-absenteeism surveillance program (e.g., by expanding existing efforts like the School-Based Active Surveillance Program or the Youth Risk Behavior Surveillance Program, which each track limited data for different goals).
- CDC should develop guidelines and funding for cities and states to expand their individual syndromic surveillance capabilities. Achieving uniformity across the nation is a major difficulty with expanding the NSSP, and CDC should work with the NSSP Community of Practice to develop, then promote, best practices through partnership with jurisdiction-specific syndromic surveillance.
To improve forecasting capabilities of health impacts:
- Congress should fund the CDC to expand its Center for Forecasting and Outbreaks Analytics (CFA) to include forecasting of environmental conditions and their health impacts. The HeatRisk service is exactly the kind of program that should also be available for smoke and cold—it clearly integrates the best science of health impacts of extreme weather events with best practices for public communications.
- Congress should fund the CDC to expand the CFA to make forecasts of operational needs for hospitals. Many hospitals now operate on a just-in-time system of stocking medical equipment that relies on typical-use rates that rapidly change during an extreme-weather event. A key piece of this operational forecasting should include potentials for cascading failures, as extreme-heat-caused failure of the electric grid is predicted to have major cascading failures in the health system.
To improve the ability to track health impacts:
- CDC should develop guidance and training on reporting environmental conditions as contributing factors on death certificates, similar to their toolkit on Death Scene Investigation After Natural Disaster or Other Weather-Related Events and other existing training. The guidance and training could be developed by analyzing existing practices from across the county. Additional training for medical providers are listed in a separate memo.
- CDC’s National Center for Environmental Health, as part of their Disaster Epidemiology and Response program, should develop guidance for states on reporting heat-related deaths to the National Vital Statistics System that includes information about how free-form text from medical examiners is coded by state-level health officials. This recommendation builds on the prior recommendation—both are needed to ensure that heat-related deaths are appropriately counted at the national level.
- CDC should expand its use of excess-death and flu-burden methods to provide official estimates of the health impacts attributable to extreme heat beyond those reported on death certificates. Such methods exist and have been used for heat; they should be standardized and regularly applied at the federal level.
- CDC should work with the Environmental Protection Agency (EPA) to expand its BenMAP software to include official estimates of health impacts attributable to extreme heat. The current software provides official estimates of health impacts attributable to air pollution and isused widely in policy. Specifically, EPA should expand its BenMAP software to: (1) include the ability to model deaths due to heat and cold and their consequences (e.g., wildfires, industrial accidents); (2) add the capability to run in real time on real-time environmental data feeds; (3) include forecasting in the tools based on short-term forecast feeds and longer-term climate models; (4) integrate the outputs as a health-impact “nowcast” available with other data feeds such as the Heat and Health Tracker, the Heat Related EMS Activation Surveillance Dashboard, and/or the HeatRisk tool.
- Develop an extreme weather event impact self-report tool and database similar to the USGS “Did You Feel It?” web-based local data collection system. The resulting qualitative data will permit more in-depth understanding of the personal, family, community, and health system impacts of weather-related emergencies.
- Several actions are needed to support the preceding recommendation, including additional interagency (EPA/CDC/National Oceanic and Atmospheric Administration (NOAA)) collaboration and data sharing. Research is needed to develop the health-impact functions for the BenMAP tool, which could be solicited in a research call such as through National Institutes of Health (NIH) Climate and Health initiative, conducted by CDC epidemiologists, or tasked to a national lab. Additional software development is also needed to cover real-time and forecast impacts in addition to the historic impacts it currently covers.
Recommendation 2. Improving Patient Care
To integrate environmental conditions into EHRs nationwide:
- Environmental conditions should be integrated with EHRs as part of data modernization efforts within federal medical providers. Examples include the Federal Electronic Health Record Modernization program and Veterans Health Administration (VHA) EHR modernization effort.
- The major EHR providers should pilot the incorporation of environmental data into EHRs beyond the federal medical systems. University medical centers would be ideal test partners for this before expansion to all hospitals nationwide.
- Federal agencies promoting the uptake of EHRs, such as the Centers for Medicare and Medicaid Services (CMS) Promoting Interoperability Program, should include the integration of environmental data in electronic health records in the tools they promote.
- CDC should add “Tracking Disasters” as a key priority in its Data Modernization Initiative and use that program to encourage tracking of disaster-relevant data, such as environmental conditions, along with health records.
To support patients during extreme heat:
- Expand the definition of medical devices to include items that protect against extreme weather. For example, air-conditioning units and other strategies that reduce personal risk of heat illness should be eligible for purchase with health savings accounts and with Medicare/Medicaid.
Conclusion
Deaths from extreme conditions, already high, are forecast to increase in the coming years and decades and potentially define a new modern era. It is vital to prepare our health system for these threats, including accurate accounting of their toll, and better prepare healthcare providers and the public for the conditions they will face.
This idea of merit originated from our Extreme Heat Ideas Challenge. Scientific and technical experts across disciplines worked with FAS to develop potential solutions in various realms: infrastructure and the built environment, workforce safety and development, public health, food security and resilience, emergency planning and response, and data indices. Review ideas to combat extreme heat here.
While some emergency care providers might be aware of the extreme weather events unfolding outside and therefore be prepared to treat related illness, the situation can change during lengthy shifts, leaving them less well prepared. This disparity between patient exposure and provider expectations can be even greater in rural areas, where patients might travel significant distances and across diverse terrain such that their exposure differs from conditions at the medical facility.
Time is also a factor. For longer-term impacts like asthma complications that could be related to smoke waves, a medical provider might be unaware that a patient experienced heavy smoke and be less able to diagnose the resulting respiratory issues
Leveraging Federal Post-Disaster Recovery Reform for Extreme Heat Adaptation and Innovation
Extreme heat is the leading weather-related cause of death in the U.S., yet it has never been the cause of a federal disaster declaration. This is because heat events are not explicitly recognized as a cause for disaster declarations under the Stafford Act, which defines federal disaster response activities. This renders those impacted by extreme heat ineligible for the substantial federal funding provided to communities that receive the official disaster declaration. A congressional amendment to the Stafford Act, and related post-disaster guidance, explicitly identifying extreme heat as an eligible disaster, would create significant opportunities for planning, funding, and implementing long-term heat adaptation while prioritizing the most physically and socially vulnerable communities.
While an extreme heat occurrence or heat wave may cause loss of life or labor, most disasters only receive federal declarations if they have excessive economic damage, property damage, and devastation beyond the capacity of a state government, which is less common in a heat event. Thus, amending the Stafford Act would assist the communities placed at an acute disadvantage in recovering and mitigating future heat events in comparison to those impacted by other extreme weather events. Likewise, it would increase U.S. capacity to address the growing challenges from increasingly frequent and extensive extreme heat events.
An extreme heat disaster declaration, followed by an appropriation from Congress, can unlock federal adaptation funding through the Department of Housing and Urban Development (HUD) Community Development Block Grants for Disaster Recovery (CDBG-DR) and Mitigation (CDBG-MIT), as well as the Federal Emergency Management Agency (FEMA) Hazard Mitigation Grant Program (HMGP). Leveraging these programs for heat adaptation, coupled with an expansion of existing proactive resilience programs such as FEMA’s Building Resilient Infrastructure and Communities, would catalyze heat adaptation planning and innovation across the country.
Challenge and Opportunity
Between 2011 and 2021, 90% of U.S. counties experienced a major disaster due to an extreme weather event. Over that period, not a single disaster declaration was made in response to an extreme heat event; yet, communities suffered from the impacts of extreme heat. Two of the states with the lowest number of disaster occurrences, Nevada and Arizona, had the highest number of deaths from heat-related illnesses between 2018 and 2021, highlighting a major flaw in the federal disaster assistance programs’ ability to protect all communities bearing the impacts of climate change. Over those four years, heat has been among the causes of death for 571 people in Nevada and 1,298 people in Arizona. That’s 4.54 and 4.46 deaths per 100,000 residents, respectively – compared to the U.S. average of 0.35 per 100,000 residents over the same period. Additionally, deaths caused by extreme heat are likely undercounted, as there are no comprehensive or consistent mechanisms for healthcare providers to track or report heat-related deaths.
In addition to being linked to growing mortality rates, extreme heat magnifies health, social, and economic disparities. According to the Centers for Disease Control (CDC), vulnerable populations — including older adults, infants and children, those with chronic conditions, lower-income individuals, athletes, outdoor workers, and pregnant people — are disproportionately affected by increased heat. Additionally, within cities, areas with less green space, often predominated by BIPOC or low-income communities, are likely to experience greater exposure to extreme heat, with higher rates of adverse outcomes. Increased and prolonged heat events also have economic impacts. Under baseline climate conditions, the United States could lose an average of approximately $100 billion annually from heat-induced lost labor productivity, which could double to nearly $200 billion by 2030 and reach $500 billion by 2050. This includes loss of agriculture due to lower labor productivity and lower crop yields.
With 2023 breaking the record as the hottest year in recorded history, the United States must urgently reform its disaster assistance policies to incorporate extreme heat through an amendment to the Stafford Act and related post-disaster guidance. Currently, the majority of adaptation funding in the United States is tied to post-disaster recovery programs, meaning communities often do not have access to resources to plan ahead unless they have already suffered. Incorporating extreme heat would open new doors for heat mitigation and adaptation for affected communities through FEMA’s HMGP, as well as HUD’s CDBG-DR and CDBG-MIT.
Plan of Action
Congress, FEMA, HUD, and the White House all have a role to play to optimize post-disaster funding and policies to address the growing challenges from excessively high temperature days and extended heat patterns.
Congress: Amendment to the Robert T. Stafford Act to Explicitly Identify Heat Events
A congressional amendment to the Stafford Act would ensure a heat event is considered an eligible event for a major disaster declaration, removing any doubt around its eligibility in perpetuity. Section 102 part (2) of the Stafford Act should be amended to:
Any natural catastrophe (including any hurricane, tornado, storm, high water, wind-driven water, tidal wave, tsunami, earthquake, volcanic eruption, landslide, mudslide, snowstorm, drought, extreme heat or cold temperature, or extended heat or cold wave), or, regardless of cause, any fire, flood, or explosion, in any part of the United States, which in the determination of the President causes damage of sufficient severity and magnitude to warrant major disaster assistance under this Act to supplement the efforts and available resources of States, local governments, and disaster relief organizations in alleviating the damage, loss, hardship, or suffering caused thereby.
FEMA: Build Heat Adaptation Capacity through Heat Disaster Response and Planning
The HMGP is a critical resource for communities that have received a presidential disaster declaration to reduce future risk to lives and property from climate hazards. An amendment to the Stafford Act to address heat eligibility would enable state and tribal governments to request HMGP funding to support extreme heat response activities, such as cooling centers, air conditioners, utility vouchers, surge capacity support for hospitals, and direct interventions for vulnerable populations. Likewise, governments could request funding under HMGP for infrastructure upgrades, including increased tree canopy, green infrastructure, cool pavement, reflective roofs, retrofitting buildings with improved HVAC systems and materials that reflect solar energy to keep indoor temperatures cooler, and power grid enhancements.
Within the HMGP, increased set-asides should be given to planning-related activities to build capacity among communities across America. Doubling funding for planning-related activities from 7% to 14% of the recipient’s HMGP funding would create greater opportunities for state, tribal, territorial, and local governments to conduct activities to strengthen their extreme heat preparedness and response, through eligible activities such as:
- Enhancing the current FEMA-approved mitigation plan by incorporating underserved and highly vulnerable populations in the planning process, risk assessment, and mitigation strategy, namely seniors, the unhoused, agriculture workers, and children.
- Integrating extreme heat adaptation information/targets from the hazard mitigation strategy into other pre- and post-disaster recovery plans, comprehensive planning, capital improvements, economic development, resource management, or other long-term community planning.
- Building capability through delivery of technical assistance and training, particularly through green infrastructure and cooling infrastructure workforce development, as well as community education on heat adaptation strategies to prevent physical and financial losses from future heat events.
- Evaluating the adoption/implementation of codes and ordinances that reduce risk to extreme heat with a focus on improvements to building codes to improve heat resilience.
Leveraging FEMA’s HMGP will bolster communities’ heat disaster response while shifting investments toward long-term disaster mitigation planning. Coupling FEMA’s HMGP funding for extreme heat planning with an expansion of FEMA’s Building Resilient Infrastructure and Communities (BRIC) would further enable communities to get ahead of the next disaster, before people suffer. FEMA made a total of $2.26 billion available through BRIC in 2022, and $1 billion in 2023. Meanwhile, the United States experienced 18 separate weather and climate disasters costing at least $1 billion in 2022 and 28 separate events in 2023. To meet the rising demands for proactive planning, FEMA must increase funding allocations for BRIC and prioritize projects that address multiple hazards.
White House: Launch a Heat Adaptation Design Challenge under the America COMPETES Act
Under the authority of the America COMPETES Act, the White House should launch a time-bound interdisciplinary planning and design challenge that brings together lived and professional expertise from local, national, and international participants to catalyze community-level long-term climate adaptation and land-use changes for communities in the United States. This model builds on the precedent set by the Rebuild by Design Hurricane Sandy Design Competition and the National Disaster Resilience Competition.
In 2013, in response to the devastation wrought by Hurricane Sandy, President Obama’s Hurricane Sandy Recovery Task Force and HUD set a new precedent for disaster recovery by launching the Hurricane Sandy Rebuild by Design Competition. The competition, authorized under the America COMPETES Act, set aside almost $1 billion of CDBG-DR funds to launch a nine-month-long interdisciplinary planning and design challenge in the Sandy-impacted region. The competition resulted in seven winning designs, which now have over $4.3 billion invested in them. The Rebuild by Design competition raised the bar for government collaboration with communities in the development of adaptation solutions, demonstrated that innovative ideas attract more dollars, and cast the region center stage of global climate adaptation solutions, attracting local, regional, and international talent. The model was subsequently used in the National Disaster Resilience Competition and the Bay Area Resilient by Design Challenge. These processes have paved the way for reimagining communities to withstand and thrive among growing climate shocks and stressors, while raising the bar for education and collaboration with impacted communities.
To date, a design challenge process has not been used to the same scale to directly address extreme heat adaptation with the support of federal funding. An interdisciplinary design challenge poses a unique opportunity to mobilize planning and design across multiple aspects that contribute to heat mitigation and adaptation, including building and road materials, energy use and storage, land use, architecture, landscape architecture, and engineering while centering the voices of impacted communities. The process could incubate innovative designs like blue-green infrastructure, social infrastructure, and community planning, as well as innovative policies such as tenant protections, energy regulations, and working standards, thereby centering people over property in disaster recovery and propelling the United States to the forefront of the global discourse on adaptation.
A national challenge would create opportunities to incubate (1) exemplary models of comprehensive heat adaptation planning, (2) sector-specific models that agencies could use to guide new and existing grant programs, and (3) heat-adaptive technologies.
- Few exemplary models of comprehensive extreme heat adaptation exist in the United States. Only a few governments – namely, Miami-Dade County, the city of Los Angeles, the city of Phoenix, the state of Arizona, and the state of Maryland – have taken great strides to mitigate the loss of life and economic output from extreme heat events by appointing chief heat officers. As a result, when tasked with taking action to mitigate extreme heat, localities are drawing from a limited toolbox of solutions, often air conditioners and cooling centers. A design competition could spur new ideas for transforming a locality’s physical spaces, including housing, transportation, right of way, parks, and public amenities to reduce risk during extreme heat, address other climate hazards, and provide needed social benefits to communities.
- Federal agencies play a key role in deploying funding to improve infrastructure across the United States. A national design challenge with a focus on heat adaptation could catalyze innovative sector-specific solutions that agencies could model in new and existing grant programs. For example, a design challenge that focuses on rethinking public right of way infrastructure to mitigate extreme heat would result in an array of outputs (research, designs, and projects) from which agencies could base new grant criteria. Similarly, this model could be used to specifically incubate ideas for housing, energy, transportation, and agriculture.
- The America COMPETES Act improves the competitiveness of the United States through investments in research and technology. A national research and design competition, focused on generating new technologies for communities, households, and individuals to adapt to heat, could seed a new industry in the United States. As rising global temperatures increasingly impact communities around the world, these technologies could thrust the United States to the forefront of global heat adaptation solutions and create domestic jobs and exports. Moreover, these interventions could reduce suffering and save countless American lives.
HUD: Heat Adaptation Planning through CDBG-DR and CDBG-MIT Funds
HUD’s CDBG-DR and CDBG-MIT funds are critical to helping communities recover from an extreme climate event in a way that better prepares them for future events; however, they are not being fully utilized to address extreme heat. These funds are only available to communities that have received a major disaster declaration. The Rebuild by Design Hurricane Sandy Design Competition and the National Disaster Resilience Competition were made feasible through allocations of CDBG-DR funds by HUD to explicitly plan ahead for future impacts from climate change, as opposed to replacing what had previously existed. An amendment to the Stafford Act to create eligibility for heat disasters would allow for an extreme heat design challenge to be supported through an appropriation of HUD CDBG-DR or CDBG-MIT funds in response to a major disaster declaration. A federally funded design challenge would also attract local and international expertise, as well as local governments, as participants would know upfront that there is implementation funding. Furthermore, the funding criteria for all disaster declarations should require that applicants assess heat vulnerability using FEMA’s Risk Rating Index or localized data to prioritize multi-hazard solutions and ensure that all disaster recovery efforts are also incentivized to address heat mitigation.
To further optimize HUD’s funding for disaster recovery and long-term planning, Congress must permanently authorize CDBG-DR. Currently, HUD allocations for CDBG-DR are slow to reach communities. Permanent authorization would remove delays and create greater predictability and certainty for communities to address the loss of life brought on by heat waves.
Conclusion
In order to address the growing challenges from extreme heat, the U.S. must dramatically shift investments from reactive disaster recovery to proactive disaster risk reduction. In the interim, making this shift will require striking down the barriers to accessing post-disaster funding for communities that need support to respond to and prepare for extreme heat by amending the Stafford Act. A national design competition, funded through post-disaster assistance, could be the mechanism to catalyze this paradigm shift by seeding innovative and exemplary heat adaptation solutions that could be modeled throughout the country. Leadership from Congress, the White House, FEMA, and HUD would ensure communities are able to respond to the impacts of today, and spur innovation and preparation for the impacts of tomorrow.
This idea of merit originated from our Extreme Heat Ideas Challenge. Scientific and technical experts across disciplines worked with FAS to develop potential solutions in various realms: infrastructure and the built environment, workforce safety and development, public health, food security and resilience, emergency planning and response, and data indices. Review ideas to combat extreme heat here.
A National Framework for Sustainable Urban Forestry to Combat Extreme Heat
Extreme heat events are increasing in frequency and intensity every year, leading to devastating human costs such as hospitalization and death. In urban environments, where over 80% of Americans live, these effects are exacerbated by the urban heat island effect. In alignment with the White House’s nature-based solutions efforts to address the effects of climate change, the role of greening has been touted as a life-saving means to protect urban residents from extreme heat, mitigate stormwater, and reduce air pollution. Nonetheless, the benefits of urban forestry have not yet been realized due to unsustainable funding at municipal levels for maintenance and stewardship, limited coordination across branches of government, inequitable distribution of trees, and a lack of analyses that define the economic value of urban forestry. A coordinated, equity-focused, and economically validated federal plan to guide the development and maintenance of urban forestry will allow the full utilization of this critical resource. Achieving this goal requires action at all levels of government; sustainable funding to grow, develop, research, and sustain urban forests; and ongoing leadership from the scientific and forestry communities.
The incoming administration should undertake a multi-agency effort to further develop the science and quantify the benefits of urban forests today and into the future. This will equip urban foresters and their municipal partners with the necessary decision support tools to plant, grow, and maintain urban forests in cities across the United States. Doing this will ensure current forestry investments created by the Inflation Reduction Act (IRA) and Bipartisan Infrastructure Law (BIL) continue to reap maximum benefits into the future. By using environmental economic principles in national accounts and leveraging the Office of Management and Budget’s (OMB) new Ecosystems Services Guidance to capture the true value of urban forests and their ecosystem services to the U.S., the federal government will provide the economic basis for further strategic planning of urban forestry. Additionally, applying the principles of environmental justice ensures decisions will support efforts to overcome the histories of redlining that prevented the expansion of urban forests into disadvantaged neighborhoods. Undertaking these efforts can lead to the realization of the potential benefits of urban forests, estimated conservatively to be over $17 billion annually.
Challenge and Opportunity
Every year, extreme heat events are increasingly threatening to human health. Recent summers have seen rises in heat-related hospitalizations. In 2023, heat-related hospitalizations increased by 51% compared to 2018. However, federal, state, and local governments are limited in their approaches to addressing extreme heat’s effect on human health and well-being. Public health approaches to tackling this growing problem include the development of coordinated messaging between public health, health systems, and community members to warn of impending extreme events, cooling centers, and the distribution of air conditioner units. Unfortunately, these prevention strategies are often reactive and unsustainable in the long term. They rely on forecasting of extreme heat events to initiate alerts or to establish cooling centers and increase demand for air conditioning, which drives up energy costs and greenhouse gas emissions.
An alternate, longer-term, and more effective strategy is to use trees as a form of natural infrastructure, particularly where the urban heat island effect takes place (i.e., the sustained increased temperatures during the day and night due to heat retention from the built environment). Trees can reduce air temperatures by up to 10ºF, and surface temperatures up to 25ºF. Urban forestry impacts over 80% of Americans, where the urban heat island effect is most pronounced. Although not accounted for in today’s macroeconomic evaluations of gross domestic product, the U.S. Department of Agriculture (USDA) Forest Service estimates that urban forestry currently provides over $17 billion in ecosystem service benefits annually through improvements in air quality, stormwater management, improved physical and mental health, and increased property values. Moreover, urban forestry is cost-effective: for every $1 spent on urban tree management, benefits are estimated to be valued at $1.37 to $3.09. Urban forests, when strategically planted or naturally regenerated and maintained, also have the potential to be a long-term, sustainable, nature-based solution to the rising threat of extreme heat on human health.
The USDA US Forest Service is rapidly expanding tree inventories across the nation, informed by the Ten-Year Urban Forestry Action Plan created by the National Urban and Community Forestry Advisory Council (NUCFAC). Funds for urban forestry have recently been appropriated through the IRA and BIL, which allocated over $1 billion over the next five years to urban forestry. Strategically channeling these funds through federal oversight and technical assistance to address the rising threat of extreme heat will provide the best opportunity to maximize the use of these funds and demonstrate the outcomes of sustaining federal investment at that scale.
Therefore, to reduce extreme heat in urban areas where most Americans live, a comprehensive urban forestry strategy is essential. This strategy should provide ongoing support within and across cities, and link the science of tree selection, climate-resilient seed propagation, planting, and maintenance with efforts to overcome disparities in urban greening infrastructure. Further, there is an ongoing need to develop the urban forestry workforce and capacity necessary to sustain these investments and ensure their benefits come to fruition. Finally, ongoing research and analysis is needed (anticipated at $50 million annually by NUCFAC) to inform urban and community forestry policy and increase the effectiveness and benefits of greening interventions.
Plan of Action
Creating a strategic plan for urban forestry management to combat extreme heat requires equity-centered coordination across various federal agencies, given the clear disparities in urban greening infrastructure within and across U.S. cities. The strategy must also further the development of research to maximize ecosystem services, incorporating the costs of urban forests over extended periods.
Thus, the federal plan of action must be guided by the following principles:
- Placing environmental justice and equitable urban greening practices at the forefront of a strategic plan.
- Employing natural capital cost assessments — a key endeavor of the Biden Administration to include environmental-economic appraisal of nature-based solutions — in the development of the potential of public-private partnerships (e.g., US Forest Service Public-Private Partnership Strategy).
- Specifying cross-agency collaboration to directly quantify the benefits from a diverse range of perspectives. For example, direct healthcare benefits from urban forestry require long-term and causal research on the quantity, distribution, and duration to account for such benefits from an environmental-economic perspective.
Coordinate the Executive Branch. A federal interagency task force consisting of urban forestry experts, healthcare authorities, economic stewards, and heat science specialists should lead the effort to create a national urban forestry strategic plan. This taskforce should be co-led by OMB and the Council on Environmental Quality (CEQ) and should include the following agencies: the USDA Forest Service, Department of the Interior (DOI), Centers for Disease Control and Prevention (CDC), National Institutes of Health (NIH), Department of Commerce Bureau of Economic Analysis, Housing and Urban Development (HUD), Department of Transportation (DOT), the National Oceanic and Atmospheric Agency (NOAA), and other agencies as relevant. The following courses of action should be taken:
- Direct studies to evaluate and directly quantify the ecosystem services and disservices of urban forestry under current and future climate scenarios.
- Dedicate resources to expeditiously create a national inventory of urban forests, indexed by location, species, and age.
- Direct agencies to build methodologies as a first case study to detail how natural capital assessments for nature-based solutions can be undertaken.
- Build a strategic plan for tree planting and maintenance by climate region and city type, including the development of decision support tools for state and city-wide urban foresters to best allocate resources.
- Undertake evaluative work to direct already appropriated funds through the IRA and BIL to urban forestry projects with the highest benefit to communities locally and regionally.
Strengthen the Evidence Base. Empirical data to inform natural capital assessments and the beneficial and detrimental effects on heat mitigation and stormwater mitigation will be required to better analyze and build policies. Areas in need of development include: human health benefits and healthcare return on investment; climate and resilience, especially around forest vulnerabilities; and environmental justice, including lowering the burden of ongoing maintenance on communities. Through the NIH, CDC, National Science Foundation (NSF), Department of Energy (DOE), Environmental Protection Agency (EPA), USDA, NOAA, and National Aeronautics and Space Administration (NASA), funding should be allocated to:
- Undertake studies to quantify and evaluate health-related ecosystem services and disservices of urban forestry under various climate scenarios in the short and long term (NIH, CDC, USDA).
- Quantify the correlation between increased greening and lower air temperatures, reductions in energy demand, benefits to energy efficiency of buildings and homes, and decreases in greenhouse gas emissions (EPA, DOE, NOAA, NASA, USDA).
- Examine the differential impacts of urban forests according to the principles of environmental justice (NIH, USDA, EPA, NSF).
- Determine the future-proofing needs of urban forestry investments across the U.S.’s 12 climatic regions (USDA, NOAA, NASA).
- Reexamine existing correlative studies to determine underlying causation regarding urban forestry human health benefits and ecosystem impacts (CDC, NSF, EPA, USDA).
- Undertake implementation studies to ensure the feasibility, cost, and efficacy of an urban forest intervention to limit the effects of extreme heat on communities (USDA, NOAA, NIH, NASA).
Conclusion
Extreme heat events are rising in intensity, frequency, and severity, particularly within cities. Existing measures to protect residents against the scourge of these events are limited while they need to be equity-focused, sustainable, and address the rising threat of climate change now and into the long term. The influx of investment in urban forestry from the IRA and BIL has provided the necessary foundation for the benefits of urban forestry as a source of nature-based solutions to combat extreme heat.
A federal strategic plan for urban forestry management to combat extreme heat is necessary to fully capture the benefits of this investment. By employing natural capital assessments, directing cross-agency collaboration, and building the necessary scientific evidence, urban forestry can serve as key infrastructure to create climate resilient communities across the United States.
This idea of merit originated from our Extreme Heat Ideas Challenge. Scientific and technical experts across disciplines worked with FAS to develop potential solutions in various realms: infrastructure and the built environment, workforce safety and development, public health, food security and resilience, emergency planning and response, and data indices. Review ideas to combat extreme heat here.
This proposal builds on the existing national Ten-Year Urban Forestry Action Plan as outlined by the National Urban and Community Forestry Advisory Council. Specifically, this proposal seeks to utilize the specific cooling effects of trees as a key ecosystem service to offset the already known risks of heat in urbanized locations.
UCF and NUCFAC are well-equipped to understand and implement the nuances of planting, maintaining, and stewarding urban forests. However, the specific health benefits of trees, the calculation of the economic benefits through natural capital assessments, and their ongoing maintenance through municipal bodies and communities require expertise and reach from a greater range of agencies. NUCFAC in particular is an advisory committee, authorized under the Federal Advisory Committee Act, and receives only a small annual budget.
For example, the impact of urban trees on the risks of heat-related mortality, hospitalization, or emergency room presentation is currently unclear. Such questions require input from health authorities combined with expertise from climatologists who can predict the effect of trees today and in the future as young trees grow, mature, and provide the greatest protection against heat through canopy coverage and evapotranspiration.
Federal administration is necessary because substantial parts of urban forests are managed on public lands, including natural areas (e.g., parks) and street trees that grow alongside thoroughfares.
Furthermore, diversity of urban forest management is necessary. The nativity and biodiversity of urban forests in the U.S. is important for preventing the spread of disease and invasive species. Managing urban forests across the different parts of the United States requires federal oversight to ensure that financial, tree planting (e.g., sapling nurseries), and tree maintenance (e.g., early tree age stewardship) resources are directed to areas of the greatest need where the effects of extreme heat are particularly threatening.
Optimizing $4 Billion of Low-Income Home Energy Assistance Program Funding To Protect the Most Vulnerable Households From Extreme Heat
The federal government needs to maximize existing funds to mitigate heat stress and ensure the equitable distribution of these resources to the most vulnerable households. Agencies could increase Low Income Home Energy Assistance Program (LIHEAP) funding allocations through incentives or by mandating a floor of benefits from these programs be distributed to a well-defined set of vulnerable households. This approach is similar to Justice40, the Biden administration’s signature environmental justice initiative that requires federal agencies to ensure a minimum allocation of 40% of program benefits are received by disadvantaged communities.
Challenge and Opportunity
In addition LIHEAP, which is administered by the Department of Health and Human Services (HHS), Justice40 covered programs with high potential to mitigate heat stress include:
- American Climate Corps (Corporation for National & Community Service, CNCS)
- Greenhouse Gas Reduction Fund (GGRF; EPA)
- Energy Efficiency and Conservation Block Grants (EECBG; DOE)
- Weatherization Assistance Program (WAP; DOE)
- Building Resilient Infrastructure and Communities (BRIC; FEMA)
LIHEAP and these five priority programs have combined allocations of about $30 billion in 2024 alone. Allocating even 10% of this collective budget to the most vulnerable communities and households could significantly reduce heat mortality and morbidity.
Since its inception in 1974, LIHEAP has provided more than $100 billion in direct bill payment assistance, more than double the allocation of seven other low-income energy programs combined. LIHEAP provides a formula block grant to all states and territories and more than 150 tribes. The FY24 LIHEAP allocation is $3.6 billion; state allocations vary depending on overall and low-income population and climate.
LIHEAP is disbursed by the HHS Administration for Children and Families (ACF) to state-level HHS counterparts. These in turn distribute funding to subgrantees, including local HHS offices, national NGOs, and community-based organizations. Furthermore, there is often coordination between state and local LIHEAP administrators and utilities, which provide additional low-income energy efficiency, solar and storage programs, and rate discounts.
HHS understands the impetus for LIHEAP to reduce heat stress. For instance, in 2021, HHS published a “Heat Stress Flexibilities and Resources” memo, which outlined the disproportionate impacts of future heat conditions on communities of color and recommended using a portion of the state allocation for cooling assistance, providing or loaning air conditioners, targeting vulnerable households, and a range of public educational activities. In 2016, the agency designated a national Extreme Heat Week on how LIHEAP can be a part of the solution.
LIHEAP Formula Funding Favors Heating Assistance
However, LIHEAP funds have not been sufficiently used for cooling assistance. Nationally, from 2001 to 2019, just 5% of all LIHEAP funds were used for cooling assistance, with heating receiving ten times more funding than cooling. Even among states in the Southeast, just 14% of the budget was for cooling assistance. In 2019, only 21 states opted to provide cooling assistance, compared to the 49 that allocated funding to weatherization and 26 that used LIHEAP for energy education and supplemental energy efficiency programs.
Some states with the highest heat risk — such as Missouri, Nevada, North Carolina, and Utah — offer no cooling assistance funds from LIHEAP. Despite their warm climates, Arizona, Arkansas, Florida, and Hawai’i all limit LIHEAP cooling assistance per household to less than half the available heating assistance benefit.

Prior efforts to encourage the use of LIHEAP for cooling have not resulted in a sufficient shift of this landmark funding source. LIHEAP was originally developed to provide home heating assistance at a time when winters were more severe and summers less searing. State LIHEAP administrators used the vast majority of their budgets during the heating season; many viewed cooling assistance as a luxury. This is despite the extreme heat events of recent summers, including temperatures topping 115ºF in the Pacific Northwest in 2019 and 31 days in a row of highs above 110ºF in Phoenix in 2023.
With many households still struggling to pay their winter bills, LIHEAP administrators may be reluctant to shift allocations from heating assistance that already cannot serve even 50% of eligible households. States that do not set aside dedicated cooling assistance funds frequently run out of LIHEAP, which they receive in October, well before summer. Even if crisis funds could theoretically be used to support families in crisis during heat waves, these funds are exhausted by high crisis demand in winter.
The majority of LIHEAP allocations are based on a formula rooted in a state’s low-income population, energy costs, and the severity of a state’s winter climate (its heating degree days). Residential energy costs may account for the number of cooling degree days, but they do not account for variation in electricity prices and have no consideration of population sensitivity (e.g., age) or adaptive capacity measures that are included in many Heat Vulnerability Indices (HVIs).
LIHEAP’s website on extreme heat points to the 2021 “heat dome” in the Pacific Northwest, which saw daily hospitalizations 69 times higher than the same week in 2020. In Washington state alone, 441 people died. The event, previously thought to be a 1 in 1,000-year occurrence, could occur every 5 to 10 years with just 2℃ of global warming (2023 was 1.35℃ warmer than the preindustrial average).
With advanced forecasts, LIHEAP could be deployed both to restore disconnected electric service and to make payments on extreme energy bills, which may surge even higher with the increase in demand response pricing. In Michigan, for example, DTE Energy offers a dynamic peak pricing rate that has critical peak periods at $1.03 per kWh, eight times higher than its off-peak rate. Maximum demand for electricity for continuous cooling coupled with time-of-use rate structures is a recipe for exorbitant bills that low-income customers will not be able to afford.
The risk to vulnerable households from the absence of cooling assistance is compounded by a lack of disconnection protections from extreme heat. Forty-one states offer protections for cooling, compared to just 20 that prevent utilities from disconnecting households during extreme heat. Heat protections often only kick in when a specific temperature is reached (e.g., 95°F) or even when a particular alert is issued by the National Weather Service, leaving households uncertain about their status.
In the bi-weekly Pulse Survey of the U.S. Census (June 28 to July 10, 2023, the most recent period of extreme heat nationally), 58.5% of national respondents reported keeping their home at an uncomfortable or unsafe temperature at least some months in the last year, with 18.7% reporting these indoor temperatures almost every month. Households that spend more of their income on energy bills allow indoor temperatures to rise up to 7.5°F more than higher-income households before using air-conditioning, thus dramatically increasing their risk of heat stress.
Plan of Action
Recommendation 1. Maximize LIHEAP funding for cooling assistance
Congressional mandate – Congress could require states to use a specific percentage of their LIHEAP allocations for cooling. This percentage could be derived from FEMA’s National Risk Index (NRI), which accounts for exposure to extreme heat, the vulnerability of the population, and adaptive capacity, such as civic resources to provide emergency response. Heat Factor by First Street and Community Resilience Estimates for Heat by U.S. Census offer more granular estimates of heat vulnerability.
Incentives – LIHEAP regularly receives supplemental federal allocations (e.g. CARES Act); HHS could use these as a pool of matching funds to encourage states to leverage non-federal dollars for cooling assistance. States also have an important role to play in leveraging both public and utility funds to match and expand the impact of LIHEAP.
Emergency funds – HHS should release Emergency Contingency Funds to address extreme heat. In the 1990s and 2000s, these funds were regularly used, sometimes in excess of $700 million per year to direct cooling assistance to extreme heat events; these funds could also be used to provide cooling measures like fans, air conditioners, and insulation. These funds have been authorized but not allocated by Congress and not disbursed since 2011.
Report back to state LIHEAP administrators – Peer comparisons can be a powerful source of information and motivation. A study from the 1990s “targeting index” for the share of LIHEAP delivered to the elderly revealed stark differences between Arizona, where the elderly were underrepresented, and Texas, where they were represented above their proportion of the population. An annual dashboard of how a state compares to its close peers (e.g., to other states in its EPA region) in cooling allocations is a low-effort step that could result in significant shifts in state plans and community outreach.
Expand outreach and education to state LIHEAP administrators and subgrantees – Memos from 2016 and 2021 were insufficient to encourage many state and local budget shifts. Communications should emphasize the significantly greater risk of fatalities from extreme heat than extreme cold. One study simulated indoor temperatures in Phoenix during the 2006 heat wave and showed that by day two, temperatures in single-story homes would peak at 115ºF (46ºC). Another study projected that a five-day heat wave on the order of the record July 2023 temperatures that corresponds with a blackout would result in a fatality rate of ~1% in Phoenix, or about 1,500 deaths.
Recommendation 2. Maximize LIHEAP distribution to the most vulnerable households
While LIHEAP providers do collect significant household data through their intake forms, most states do not have firm guidelines on which households to distribute LIHEAP funds to and use a modified first-come, first-served approach. A small number of questions specific to heat risk could be added to LIHEAP applications and used to generate a household heat vulnerability score (raw or percentile). A list of 10 potential sensitivity factors to assess is included in the Frequently Asked Questions.
In partnership with extreme heat experts, US Digital Service could support the development of an algorithm to assess the likelihood of each household experiencing acute heat stress and the optimal uses of LIHEAP funding to mitigate these threats, at the household level and portfolio-wide.
Existing data from the Community Resilience Estimates for Heat (CRE) by the U.S. Census shows that more than two-thirds of extreme heat vulnerability is concentrated in just 1.5% of U.S. census tracts across 10 states. Even a small amount of LIHEAP cooling assistance, if effectively targeted, could dramatically reduce the risk of heat stroke and death.
Recommendation 3. Congressional Amendments to the LIHEAP Statute
Congress has revisited the LIHEAP formula in the past and should consider revising the formulas to elevate the role of cooling assistance and disconnection prevention during extreme heat. Rep. Watson Coleman (D-NJ) proposed this in the Stay Cool Act introduced in 2022. As the climate has changed dramatically since LIHEAP’s inception and will continue to in coming decades, Congress could peg an updated formula to an HVI as a national standard to ensure shifts in climate and population would be automatically updated in the annual LIHEAP formula. It could also update household data collection requirements under LIHEAP Statute Section 2605(c)(1)(G).
Conclusion
The number of heat-related deaths continues to rise in the U.S. In the long term, a multipronged strategy that increases funding for energy efficiency improvements, distributed generation and storage, and bill assistance is needed. But in the near term, it is critically important to work with existing resources and maximize the value of LIHEAP to mitigate the pressures of extreme heat.
Despite some positive spikes, annual LIHEAP allocations have not kept pace with accelerating demand. The number of households eligible for LIHEAP has grown four times faster than available funding; the number of eligible households served has declined from 36% to 16%. As utility bills outpace inflation, per-household LIHEAP allocations have increased without a corresponding increase in the overall allocation.
States have broad discretion on how to use LIHEAP. Overcoming the inertia of budgets dominated by heating assistance is likely to require significant advocacy, both top-down from the federal government and bottom-up from grassroots community organizations that share concerns about vulnerability to extreme heat.
This idea of merit originated from our Extreme Heat Ideas Challenge. Scientific and technical experts across disciplines worked with FAS to develop potential solutions in various realms: infrastructure and the built environment, workforce safety and development, public health, food security and resilience, emergency planning and response, and data indices. Review ideas to combat extreme heat here.
The process to develop household heat risk assessments and performance reporting could entail:
1) Design a method for assigning household scores for heat risk. Scores might consider risk of mortality, risk of heat sickness requiring medical attention/hospitalization, and risk of chronic impacts (e.g., declines in cognition and sleep quality) from consistent, low to moderate exposure to excessive heat.
Current data: LIHEAP reporting by each state’s lead agency currently includes some data that can be used to analyze prioritization of funds to mitigate extreme heat risks:
- Cooling assistance (dollars; number of households served)
- Weatherization (funded through LIHEAP)
- Assistance distributed to households with a vulnerable person (under age 5, over age 60, or a person with a disability)
- Demographic variables (e.g. race and ethnicity)
- Housing variables, namely occupancy status and for renters, whether utility bills are included in rent
- Disconnections
Proposed data collection:
- Keeping house at an unsafe temperature Medical conditions associated with heat stress (e.g., diabetes)
- Prior experience of heat stress
- Additional age distinctions (children under 2, adults over 70, over 80, over 90)
- Presence and adequacy of cooling systems Housing age and type (e.g., masonry, duplex)
- Electricity cost Solar exposure (provided by Google’s Project Sunroof)
- Urban heat island effect
- Employment
- Personal behaviors
2) Design a process so that existing program resources are distributed among the most vulnerable households, as determined by their individual heat risk scores. LIHEAP administrators might decide to spend 25% of cooling assistance funds among the most vulnerable 10% of LIHEAP applicants, for instance.
Yes, the Community Resilience Estimates for Heat (CRE) uses American Community Survey Data to determine the number of vulnerability factors a household possesses, down to census tract resolution. The tool sorts census tracts based on the number of households with zero vulnerabilities, 1–2 vulnerabilities, and 3 or more vulnerabilities. Of 73,060 census tracts, just 1,616 (2.2%) have a majority of households with more than three heat vulnerabilities. The Community Resilience Estimates (CRE) for Heat offers 10 binary risk factors.
Enhancing Public Health Preparedness for Climate Change-Related Health Impacts
The escalating frequency and intensity of extreme heat events, exacerbated by climate change, pose a significant and growing threat to public health. This problem is further compounded by the lack of standardized education and preparedness measures within the healthcare system, creating a critical gap in addressing the health impacts of extreme heat. The Department of Health and Human Services (HHS), especially the Centers for Medicare & Medicaid Services (CMS), the Health Resources and Services Administration (HRSA), and the Office of Climate Change and Health Equity (OCCHE) can enhance public health preparedness for the health impacts of climate change. By leveraging funding mechanisms, incentives, and requirements, HHS can strengthen health system preparedness, improve health provider knowledge, and optimize emergency response capabilities.
By focusing on interagency collaboration and medical education enhancement, strategic measures within HHS, the healthcare system can strengthen its resilience against the health impacts of extreme heat events. This will not only improve coding accuracy, but also enhance healthcare provider knowledge, streamline emergency response efforts, and ultimately mitigate the health disparities arising from climate change-induced extreme heat events. Key recommendations include: establishing dedicated grant programs and incentivizing climate-competent healthcare providers; integrating climate-resilience metrics into quality measurement programs; leveraging the Health Information Technology for Economic and Clinical Health (HITECH) Act to enhance ICD-10 coding education; and collaborating with other federal agencies such as the Department of Veterans Affairs (VA), the Federal Emergency Management Agency (FEMA), and the Department of Defense (DoD) to ensure a coordinated response. The implementation of these recommendations will not only address the evolving health impacts of climate change but also promote a more resilient and prepared healthcare system for the future.
Challenge
The escalating frequency and intensity of extreme heat events, exacerbated by climate change, pose a significant and growing threat to public health. The scientific consensus, as documented by reports from the Intergovernmental Panel on Climate Change (IPCC) and the National Climate Assessment, reveals that vulnerable populations, such as children, pregnant people, the elderly, and marginalized communities including people of color and Indigenous populations, experience disproportionately higher rates of heat-related illnesses and mortality. The Lancet Countdown’s 2023 U.S. Brief underscores the escalating threat of fossil fuel pollution and climate change to health, highlighting an 88% increase in heat-related mortality among older adults and calling for urgent, equitable climate action to mitigate this public health crisis.
Inadequacies in Current Healthcare System Response
Reports from healthcare institutions and public health agencies highlight how current coding practices contribute to the under-recognition of heat-related health impacts in vulnerable populations, exacerbating existing health disparities. The current inadequacies in ICD-10 coding for extreme heat-related health cases hinder effective healthcare delivery, compromise data accuracy, and impede the development of targeted response strategies. Challenges in coding accuracy are evident in existing studies and reports, emphasizing the difficulties healthcare providers face in accurately documenting extreme heat-related health cases. An analysis of emergency room visits during heat waves further indicates a gap in recognition and coding, pointing to the need for improved medical education and coding practices. Audits of healthcare coding practices reveal inconsistencies and inaccuracies that stem from a lack of standardized medical education and preparedness measures, ultimately leading to underreporting and misclassification of extreme heat cases. Comparative analyses of health data from regions with robust coding practices and those without highlight the disparities in data accuracy, emphasizing the urgent need for standardized coding protocols.
There is a crucial opportunity to enhance public health preparedness by addressing the challenges associated with accurate ICD-10 coding in extreme heat-related health cases. Reports from government agencies and economic research institutions underscore the economic toll of extreme heat events on healthcare systems, including increased healthcare costs, emergency room visits, and lost productivity due to heat-related illnesses. Data from social vulnerability indices and community-level assessments emphasize the disproportionate impact of extreme heat on socially vulnerable populations, highlighting the urgent need for targeted policies to address health disparities.
Opportunity
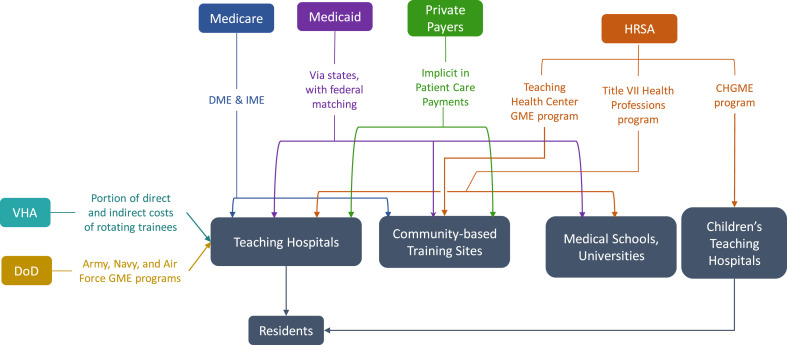
As Medicare is the largest federal source of Graduate Medical Education (GME) funding (Figure 1), the Department of Health and Human Services’ (HHS) Centers for Medicare & Medicaid Services (CMS) and the National Center for Health Statistics (NCHS) play a critical role in developing coding guidelines. Thus, it is essential for HHS, CMS, and other pertinent coordinating agencies to be involved in the process for developing climate change-informed graduate medical curricula.
By focusing on medical education enhancement, strategic measures within HHS, and fostering interagency collaboration, the healthcare system can strengthen its resilience against the health impacts of extreme heat events. Improving coding accuracy, enhancing healthcare provider knowledge, streamlining emergency response efforts, and mitigating health disparities related to extreme heat events will ultimately strengthen the healthcare system and foster more effective, inclusive, and equitable climate and health policies. Improving the knowledge and training of healthcare providers empowers them to respond more effectively to extreme heat-related health cases. This immediate response capability contributes to the overarching goal of reducing morbidity and mortality rates associated with extreme heat events and creates a public health system that is more resilient and prepared for emerging challenges.
The inclusion of ICD-10 coding education into graduate medical education funded by CMS aligns with the precedent set by the Pandemic and All Hazards Preparedness Act (PAHPA), emphasizing the importance of preparedness and response to public health emergencies. Similarly, drawing inspiration from the Health Information Technology for Economic and Clinical Health Act (HITECH Act), which promotes the adoption of electronic health records (EHR) systems, presents an opportunity to modernize medical education and ensure the seamless integration of climate-related health considerations. This collaborative and forward-thinking approach recognizes the interconnectedness of health and climate, offering a model that can be applied to various health challenges. Integrating mandates from PAHPA and the HITECH Act serves as a policy precedent, guiding the healthcare system toward a more adaptive and proactive stance in addressing climate change impacts on health.
Conversely, the consequences of inaction on the health impacts of extreme heat extend beyond immediate health concerns. They permeate through the fabric of society, widening health disparities, compromising the accuracy of health data, and undermining emergency response preparedness. Addressing these challenges requires a proactive and comprehensive approach to ensure the well-being of communities, especially those most vulnerable to the effects of extreme heat.
Plan of Action
The following recommendations aim to facilitate public health preparedness for extreme heat events through enhancements in medical education, strategic measures within the Department of Health and Human Services (HHS), and fostering interagency collaboration.
Recommendation 1a. Integrate extreme heat training into the GME curriculum.
Integrating modules on extreme heat-related health impacts and accurate ICD-10 coding into medical education curricula is essential for preparing future healthcare professionals to address the challenges posed by climate change. This initiative will ensure that medical students receive comprehensive training on identifying, treating, and documenting extreme heat-related health cases. Sec. 304. Core Education and Training of the PAHPA provides policy precedent to develop foundational health and medical response curricula and training materials by modifying relevant existing programs to enhance responses to public health emergencies. Given the prominence of Medicare in funding medical residency training, policies that alter Medicare GME can affect the future physician supply and can be used to address identified healthcare workforce priorities related to extreme heat (Figure 2).
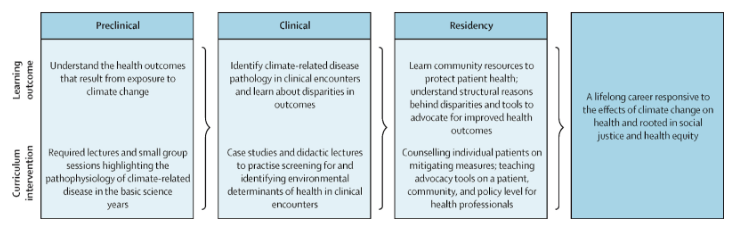
Figure 2: A model for comprehensive climate and medical education (adapted from Jowell et al. 2023)
Recommendation 1b. Collaborate with Veterans Health Administration Training Programs.
Partnering with the Department of Veterans Affairs (VA) to extend climate-related health coding education to Veterans Health Administration (VHA) training programs will enhance the preparedness of healthcare professionals within the VHA system to manage and document extreme heat-related health cases among veteran populations.
Recommendation 2. Collaborate with the Agency for Healthcare Research and Quality (AHRQ)
Establishing a collaborative research initiative with the Agency for Healthcare Research and Quality (AHRQ) will facilitate the in-depth exploration of accurate ICD-10 coding for extreme heat-related health cases. This should be accomplished through the following measures:
Establish joint task forces. CMS, NCHS, and AHRQ should establish joint research initiatives focused on improving ICD-10 coding accuracy for extreme heat-related health cases. This collaboration will involve identifying key research areas, allocating resources, and coordinating research activities. Personnel from each agency, including subject matter experts and researchers from the EPA, NOAA, and FEMA, will work together to conduct studies, analyze data, and publish findings. By conducting systematic reviews, developing standardized coding algorithms, and disseminating findings through AHRQ’s established communication channels, this initiative will improve coding practices and enhance healthcare system preparedness for extreme heat events.
Develop standardized coding algorithms. AHRQ, in collaboration with CMS and NCHS, will lead efforts to develop standardized coding algorithms for extreme heat-related health outcomes. This involves reviewing existing coding practices, identifying gaps and inconsistencies, and developing standardized algorithms to ensure consistent and accurate coding across healthcare settings. AHRQ researchers and coding experts will work closely with personnel from CMS and NCHS to draft, validate, and disseminate these algorithms.
Integrate into Continuous Quality Improvement (CQI) programs. Establish collaborative partnerships between the VA and other federal healthcare agencies, including CMS, HRSA, and DoD, to integrate education on ICD-10 coding for extreme heat-related health outcomes into CQI programs. Regularly assess the effectiveness of training initiatives and adjust based on feedback from healthcare providers. For example, CMS currently requires physicians to screen for the social determinants of health and could include level of climate and/or heat risk within that screening assessment.
Allocate resources. Each agency will allocate financial resources, staff time, and technical expertise to support collaborative activities. Budget allocations will be based on the scope and scale of specific initiatives, with funds earmarked for research, training, data sharing, and evaluation efforts. Additionally, research funding provided through PHSA Titles VII and VIII can support studies evaluating the effectiveness of educational interventions on climate-related health knowledge and practice behaviors among healthcare providers.
Recommendation 3. Leverage the HITECH Act and EHR.
Recommendation 4. Establish climate-resilient health system grants to incentivize state-level climate preparedness initiatives
HHS and OCCHE should create competitive grants for states that demonstrate proactive climate change adaptation efforts in healthcare. These agencies can encourage states to integrate climate considerations into their health plans by providing additional funding to states that prioritize climate resilience.
Within CMS, the Center for Medicare and Medicaid Innovation (CMMI) could help create and administer these grants related to climate preparedness initiatives. Given its focus on innovation and testing new approaches, CMMI could design grant programs aimed at incentivizing state-level climate resilience efforts in healthcare. Given its focus on addressing health disparities and promoting preventive care, the Bureau of Primary Health Care (BPHC) within HRSA could oversee grants aimed at integrating climate considerations into primary care settings and enhancing resilience among vulnerable populations.
Conclusion
These recommendations provide a comprehensive framework for HHS — particularly CMS, HRSA, and OCCHE— to bolster public health preparedness for the health impacts of extreme heat events. By leveraging funding mechanisms, incentives, and requirements, HHS can enhance health system preparedness, improve health provider knowledge, and optimize emergency response capabilities. These strategic measures encompass a range of actions, including establishing dedicated grant programs, incentivizing climate-competent healthcare providers, integrating climate-resilience metrics into quality measurement programs, and leveraging the HITECH Act to enhance ICD-10 coding education. Collaboration with other federal agencies further strengthens the coordinated response to the growing challenges posed by climate change-induced extreme heat events. By implementing these policy recommendations, HHS can effectively address the evolving landscape of climate change impacts on health and promote a more resilient and prepared healthcare system for the future.
This idea of merit originated from our Extreme Heat Ideas Challenge. Scientific and technical experts across disciplines worked with FAS to develop potential solutions in various realms: infrastructure and the built environment, workforce safety and development, public health, food security and resilience, emergency planning and response, and data indices. Review ideas to combat extreme heat here.
- Improved Accuracy in ICD-10 Coding: Healthcare providers consistently apply accurate ICD-10 coding for extreme heat-related health cases.
- Enhanced Healthcare Provider Knowledge: Healthcare professionals possess comprehensive knowledge on extreme heat-related health impacts, improving patient care and response strategies.
- Strengthened Public Health Response: A coordinated effort results in a more effective and equitable public health response to extreme heat events, reducing health disparities.
- Improved Public Health Resilience:
- Short-Term Outcome: Healthcare providers, armed with enhanced knowledge and training, respond more effectively to extreme heat-related health cases.
- Long-Term Outcome: Reduced morbidity and mortality rates associated with extreme heat events lead to a more resilient and prepared public health system.
- Enhanced Data Accuracy and Surveillance:
- Short-Term Outcome: Improved accuracy in ICD-10 coding facilitates more precise tracking and surveillance of extreme heat-related health outcomes.
- Long-Term Outcome: Comprehensive and accurate data contribute to better-informed public health policies, targeted interventions, and long-term trend analysis.
- Reduced Health Disparities:
- Short-Term Outcome: Incentives and education programs ensure that healthcare providers prioritize accurate coding, reducing disparities in the diagnosis and treatment of extreme heat-related illnesses.
- Long-Term Outcome: Health outcomes become more equitable across diverse populations, mitigating the disproportionate impact of extreme heat on vulnerable communities.
- Increased Public Awareness and Education:
- Short-Term Outcome: Public health campaigns and educational initiatives raise awareness about the health risks associated with extreme heat events.
- Long-Term Outcome: Informed communities adopt preventive measures, reducing the overall burden on healthcare systems and fostering a culture of proactive health management.
- Streamlined Emergency Response and Preparedness:
- Short-Term Outcome: Integrating extreme heat preparedness into emergency response plans results in more efficient and coordinated efforts during heatwaves.
- Long-Term Outcome: Improved community resilience, reduced strain on emergency services, and better protection for vulnerable populations during extreme heat events.
- Increased Collaboration Across Agencies:
- Short-Term Outcome: Collaborative efforts between OCCHE, CMS, HRSA, AHRQ, FEMA, DoD, and the Department of the Interior result in streamlined information sharing and joint initiatives.
- Long-Term Outcome: Enhanced cross-agency collaboration establishes a model for addressing complex public health challenges, fostering a more integrated and responsive government approach.
- Empowered Healthcare Workforce:
- Short-Term Outcome: Incentives for accurate coding and targeted education empower healthcare professionals to address the unique challenges posed by extreme heat.
- Long-Term Outcome: A more resilient and adaptive healthcare workforce is equipped to handle emerging health threats, contributing to overall workforce well-being and satisfaction.
- Informed Policy Decision-Making:
- Short-Term Outcome: Policymakers utilize accurate data and insights to make informed decisions related to extreme heat adaptation and mitigation strategies.
- Long-Term Outcome: The integration of health data into broader climate and policy discussions leads to more effective, evidence-based policies at local, regional, and national levels.
A Call for Immediate Public Health and Emergency Response Planning for Widespread Grid Failure Under Extreme Heat
Soaring energy demands and unprecedented heatwaves have placed the U.S. on the brink of a severe threat with the potential to impact millions of lives: widespread grid failure across multiple states. While the North American Electric Reliability Corporation (NERC), tasked with overseeing grid reliability under the Federal Energy Regulatory Commission (FERC), has issued warnings about the heightened risk of grid failures, the prospect of widespread summer blackouts looms large amid the nation’s unpreparedness for such scenarios.
As a proactive measure, there needs to be a mandate for the implementation of an Executive Order or an interagency Memorandum of Understanding (MOU) mandating the expansion of Public Health and Emergency Response Planning for Widespread Grid Failure Under Extreme Heat. This urgently needed action would help mitigate the worst impacts of future grid failures under extreme heat, safeguarding lives, the economy, and national security as the U.S. moves toward a more sustainable, stable, and reliable electric grid system.
When the lights go out, restoring power across America is a complex, intricate process requiring seamless collaboration among various agencies, levels of government, and power providers amid constraints extending beyond just the loss of electricity. In a blackout, access to critical services like telecommunications, transportation, and medical assistance is also compromised, which only intensifies and compounds the urgency for coordinated response efforts. To avert blackouts, operators frequently implement planned and unplanned rolling blackouts, a process for load shedding that eases strain on the grid. However, these actions may lack transparent protocols and criteria for safeguarding critical medical services. Equally crucial and missing are frameworks to prioritize regions for power restoration, ensuring equitable treatment for low-income and socially vulnerable communities affected by grid failure events.
Thus, given the gravity of these high-risk, increasingly probable scenarios facing the United States, it is imperative for the federal government to take a leadership role in assessing and directing planning and readiness capabilities to respond to this evolving disaster.
Challenge
Grids are facing unprecedented strain due to record-high temperatures, which reduce their energy transmission efficiency and spike demand for air conditioning during the summer. On top of this, new industries are pushing grids to their limits. The Washington Post and insights from the utility industry cite the exponential growth of artificial intelligence and data centers for cloud computing and crypto mining as drivers of a nearly twofold increase in electricity consumption over the past decade.
Projections from NERC paint a dire picture: between 2024 and 2028, an alarming 300 million people across the United States could face power outages. This underscores the pressing need for robust emergency response and public health planning.
The impact of power loss is especially profound for vulnerable populations, including those reliant on electricity-dependent medical equipment and life-saving medications that require refrigeration. Extreme heat significantly increases public health risks by exacerbating mental health, behavioral disorders, and chronic illnesses such as heart and respiratory conditions, and increasing the likelihood of preterm births and developmental issues in infants and children. Excessive temperatures also impose burdens on older adults.
Since 2015, national power outages have surged by over 150% owing to demand and extreme weather amplified by climate change. Increasing temperatures can cause transformers to overheat and explode, sometimes sparking fires and cascading outages. Other types of severe weather events, such as lightning strikes, high winds, and flying debris, further escalate the risk of utility infrastructure damage.
In 2020, 22 extreme weather events – from cyclones to hurricanes, heat, and drought – cost the U.S. a combined $95 billion. The following year, disasters like the Texas winter storm and the Pacific Northwest heatwave vividly illustrated the severe consequences of extreme weather on grid stability. To put this into perspective,
- The Pacific Northwest heatwave resulted in thousands of heat-related emergency department visits and over 700 deaths.
- During the Texas winter storm, 4.5 million customers went without power, leading to over 240 deaths and economic damages estimated at $130 billion.
These events led to rolling blackouts, thousands of heat-related emergency room visits, numerous deaths, and substantial economic losses. This remains an actively ongoing paradigm, with the National Oceanic and Atmospheric Administration’s (NOAA) 2023 Billion-dollar disaster report confirming 28 weather and climate disasters in a single year, surpassing the previous record of 22 in 2020, with a price tag of at least $92.9 billion.
Historical disasters, such as Hurricane Maria in 2017 and the Northeastern blackout in 2003, are stark reminders of the devastating impact of prolonged power outages. The aftermath of such events includes loss of life, disruptions to healthcare access, and extensive economic damages.
- Hurricane Maria affected 1.6 million people, with loss of electricity for 328 days, 4600 direct deaths – 70 times the official toll – and an estimated third more excess deaths attributed to the lack of access to health care, and an estimated $90 billion in damages.
- The Northeastern blackout impacted 30 million customers across the U.S. and Canada, causing at least 11 deaths and estimated economic losses of $6 billion.
A stark 2023 study reported that “If a multi-day blackout in Phoenix coincided with a heat wave, nearly half the population would require emergency department care for heat stroke or other heat-related illnesses.” Under such conditions, the researchers estimate that 12,800 people in Phoenix would die.
During these events, restoring power and providing mass care falls on various entities. Utility and power operators are tasked with repairing grid infrastructure, while the Federal Emergency Management Agency (FEMA) coordinates interagency actions through its National Response Framework and Emergency Support Functions (ESFs).
For example, ESF #6 handles mass care missions like sheltering and feeding, while ESF #8 coordinates public health efforts, overseen by the Department of Health and Human Services (HHS). FEMA’s Power Outage Incident Annex (POIA) enables utility operators to request support through ESF #12.While there is some testing of system responses to blackouts, few states have conducted exercises at scale, which is crucial, given the immense complexity of restarting grid infrastructure and coordinating mass care operations simultaneously.
Opportunity
The Department of Energy’s (DOE) Liberty Eclipse Program exemplifies a successful public-private partnership aimed at bolstering energy sector preparedness against cyberattacks on the grid. Similarly, FEMA conducts numerous Incident Command Systems (ICS) training annually, emphasizing collaboration across governments, nongovernmental organizations (NGOs), and the private sector.
By leveraging interagency mechanisms like MOUs, FEMA, DOE, and HHS can integrate and expand exercises addressing heat-induced grid failure into existing training frameworks. Such collaborative efforts would ensure a comprehensive approach to preparedness. Additionally, funds typically earmarked for state and local agency training could cover their participation costs in these exercises, optimizing resource utilization and ensuring widespread preparedness across all government levels.
There are also several federal policy efforts currently aligned with this proposal’s objectives, demonstrating a concerted effort to address related challenges through legislation, executive branch actions, programs, and precedents. Notable legislative initiatives, such as Rep. Ruben Gallego’s proposal to amend the Stafford Act, underscore a growing recognition of the unique threats posed by extreme heat events and the need for proactive federal measures.
Simultaneously, regulatory initiatives, such as those by FERC, signal a proactive stance in enhancing energy infrastructure resilience against extreme weather events. Building on an established precedent, FERC could direct NERC to create extreme heat reliability standards for power sector operators, akin to those established for extreme cold weather in 2024 (E-1 | RD24-1-000), further ensuring the reliable operation of the Bulk Electric System (BES).A pivotal resource informing our proposal is the 2018 report by the President’s National Infrastructure Advisory Council (NIAC), which emphasizes the significance of addressing catastrophic grid failure and underscores ongoing efforts dedicated to this pressing issue. Tasked with assessing the nation’s preparedness for “catastrophic power outages beyond modern experience,” the report offers invaluable insights and recommendations, particularly relevant to the following recommendation.
Plan of Action
To enhance national resilience, save tens of thousands of lives, and prevent significant economic losses, the National Security Council (NSC) should coordinate collaboration between implicated agencies (DOE, HHS, and FEMA) on grid resilience under extreme heat conditions and work to establish an interagency MOU to fortify the nation’s resilience against extreme heat events, with a specific focus on disaster planning for grid failure. This proposal will have minimal direct impact on the federal budget as it will use existing frameworks within agencies such as FEMA, the DOE, and HHS. These agencies already allocate resources towards preparedness training and testing, as evidenced by their annual budgets.
Recommendation 1. NSC should initiate a collaboration between DOE, HHS, and FEMA.
The NSC should direct DOE to assess grid resilience under extreme heat and coordinate and prepare for widespread grid failure events in collaboration with FEMA and HHS. This collaboration would involve multi-state, multi-jurisdictional entities, tribal governments, and utilities in scaling planning and preparedness.
Under this coordinated action, federal agencies, with input from partners in the NSC should undertake the following steps:
The DOE Office of Cybersecurity, Energy Security, and Emergency Response (CESER), in collaboration with FERC and NERC, should develop comprehensive extreme heat guidelines for utilities and energy providers. These guidelines should include protocols for monitoring grid performance, implementing proactive maintenance measures, communicating concerns and emerging issues, and establishing transparent and equitable processes for load shedding during extreme heat events. Equitable and transparent load shedding is critical as energy consumption rises, driven in part by new industries like clean tech manufacturing and data centers.
FEMA should:
- Update the National Incident Management System to include extreme heat-induced grid failure in disaster response scenarios.
- Conduct risk assessments and develop a whole community approach to emergency response and preparedness plans to address the scale of widespread, multi-state grid failure events. This is in line with FEMA’s goal to increase resilience in the face of more frequent, far-reaching, and widespread natural and manmade disasters.
- Collaborate with state, tribal, and local governments, utilities, NGOs, and other partners to identify critical infrastructure vulnerabilities and prioritize mitigation and response measures, incorporating an equity mapping component to ensure equitable distribution of resources and assistance.
HHS should strengthen functions under ESF#8 to deliver public health services during extreme heat-induced grid failure events, with enhanced coordination between the Centers for Disease Control and Prevention (CDC) and the Assistant Secretary for Preparedness and Response (ASPR).
Recommendation 2. Establish an interagency MOU
An interagency MOU should streamline coordination and collaboration on extreme heat disaster planning and preparedness for grid failure. Further, these agreements should prepare agencies to facilitate cross-sector collaboration with states and local governments through the establishment of a national task force.
This MOU should outline the following actions:
- Joint task force: Create a task force comprising lead representatives from relevant agencies and partner organizations to develop, advance, and test extreme heat-induced grid failure disaster planning and preparedness. This task force would lead efforts to formulate planning strategies, conduct disaster training exercises, and facilitate the exchange of critical information among emergency managers, public health emergency preparedness (PHEP) teams, utilities, and medical providers.
- Information sharing protocols: Develop standardized protocols for sharing data and intelligence on heatwave forecasts, grid stability alerts, and response capabilities across agencies and jurisdictions.
- Training and exercise programs: Coordinate the development and implementation of training exercises to test and improve response procedures to extreme heat events across sectors.
- Public outreach and education: Collaborate on public outreach campaigns to raise awareness about heat-related risks and preparedness measures. Disseminate existing communication tools and education programs developed for weather disasters through local agencies to enhance family and neighborhood resilience to extreme heat-induced grid failures. Special attention should be given to meeting the needs of vulnerable populations, with a strong emphasis on equity, public health, and social cohesion. Resources such as the HHS emPOWER Program Platform and ArcGIS mapping tools like the National Integrated Heat Health Information System’s (NIHHIS) “Future Heat Events and Social Vulnerability,” FEMA’s Resilience Analysis and Planning Tool (RAPT), or the CDC’s Environmental Justice and Map Dashboard offer data-driven approaches to achieve this objective.
- Community resilience: FEMA, branches of HHS, CDC, and ASPR, in collaboration with branches of the NOAA, including the National Weather Service and the NIHHIS, should work to help communities fortify their resilience against widespread blackouts during extreme heat events. Leveraging existing weather disaster resources for storms, fires, and hurricanes, resilience planning should be expanded and adapted to address the loss of electricity, water, and sanitation systems; communication breakdowns; transportation disruptions; and interruptions in medical services under extreme heat conditions.
Conclusion
This proposal emphasizes planning for blackouts and response readiness when the lights go out across wide swaths of America during extreme heat. Addressing this critical gap in federal disaster response planning would secure the safety of millions of citizens and prevent billions of dollars in potential economic losses.
An Executive Action or interagency MOU would facilitate coordinated planning and preparedness, leveraging existing frameworks and engaging stakeholders beyond traditional boundaries to effectively manage potential catastrophic, multi-state grid failures during heat waves. Specific steps to advance this initiative include ensuring no ongoing similar exercises, scheduling meetings with pertinent agency leaders, revisiting policy recommendations based on agency feedback, and drafting language to incorporate into interagency MOUs.
Using existing authorities and funding, implementing these recommendations would safeguard lives, protect the economy, and bolster national security, particularly as the U.S. moves toward a more sustainable, stable, and reliable electric grid system.
This idea of merit originated from our Extreme Heat Ideas Challenge. Scientific and technical experts across disciplines worked with FAS to develop potential solutions in various realms: infrastructure and the built environment, workforce safety and development, public health, food security and resilience, emergency planning and response, and data indices. Review ideas to combat extreme heat here.
This proposal is fully aligned with the Biden Administration’s executive actions on climate change, specifically, Executive Orders 14008 and 13990, which have led to significant initiatives aimed at addressing climate-related challenges and promoting environmental justice. These actions resulted in the establishment of key entities such as the Office of Climate Change and Health Equity at the Department of Health and Human Services (HHS), as well as in the development of the HHS’ national Climate and Health Outlook and the CDC’s Heat and Health Tracker, and heat planning and preparedness guides. Furthermore, the launch of Heat.gov and the interagency National Integrated Heat Health Information System (NIHHIS), are significant steps in providing accessible and science-based information to the public and decision-makers to support equitable heat resilience. Heat.gov serves as a centralized platform offering comprehensive resources, including NIHHIS programs, events, news articles, heat and health program funding opportunities, and information tailored to at-risk communities. This initiative underscores President Biden’s dedication to tackling the health risks associated with extreme heat and is a priority of his National Climate Task Force and its Interagency Working Group on Extreme Heat. This proposal complements these efforts and aligns closely with the administration’s broader climate and health equity agenda. By leveraging existing frameworks and collaborating across agencies, it is possible to further advance the administration’s objectives while effectively addressing the urgent challenges posed by climate change.
This policy memo was written by the Federation of American Scientists in collaboration with the Pima County Department of Health (Dr. Theresa Cullen, Dr. Julie Robinson, Kat Davis), which provided research and information support to the authors. The Pima County Department of Health seeks to advance health equity and environmental justice for the citizens of Arizona and beyond.
Protecting Workers from Extreme Heat through an Energy-efficient Workplace Cooling Transformation
Extreme heat is a growing threat to the health and productivity of U.S. workers and businesses. There is a high-impact opportunity to pioneer innovations in energy-efficient worker-centric cooling to protect workers from the growing heat while reducing the costs to businesses to install protections. With the impending Occupational Safety and Health Administration (OSHA) standard, the federal government should ensure that businesses have the necessary support to establish and maintain the infrastructure needed for existing and upcoming worker heat protection requirements while realizing economic, disaster resilience, and climate co-benefits. To achieve this goal, an Executive Order should form a multiagency working group that coordinates federal government and nongovernment partners to define a new building design approach that integrates both worker health and energy-efficiency considerations. The working group should establish roles and a process for coordinating and identifying leaders and funding approaches to advance a policy roadmap to accelerate, scale up, and evaluate equitable deployment and maintenance of energy-efficient worker-centric cooling. This plan presents a unique and timely opportunity to build upon existing national clean energy, climate, and infrastructure commitments and goals to ensure a healthier, more productive, resilient, and sustainable workforce.
Challenge and Opportunity
U.S. workers and businesses face a growing threat of illness, death, and reduced work productivity from extreme heat exposure. There were 436 work-related heat deaths recorded in the U.S. from 2011 to 2021. Workplace heat exposure is linked to heat illnesses, traumatic injuries, and reduced work productivity among otherwise healthy workers, costing the nation an estimated $100 billion each year in lost economic activity. Workers exposed to high heat include those in outdoor occupations in agriculture and construction and those working in hot manufacturing, transportation and warehousing, and food services environments. Spikes in worker heat illness have occurred during recent extreme heat events, such as the “heat dome” event of 2021, which are more likely to occur with climate change. Disproportionately exposed workers and small businesses often do not have the resources or capacity to implement, improve, or maintain existing workplace cooling infrastructure, thus increasing heat exposure inequities.
An energy-efficient workplace cooling transformation is needed to ensure businesses have the support required to comply with existing state heat rules and upcoming federal workplace heat prevention requirements. Several states—California, Colorado, Oregon, Minnesota, and Washington—have already adopted occupational indoor and/or outdoor heat exposure rules to protect workers from heat stress. OSHA is in the process of developing a national workplace heat standard. In addition to requirements for worker rest breaks, training, and hydration, OSHA is considering requirements for employers to implement protections when the measured heat index is 80°F or higher, including engineering controls such as air-conditioned cool-down areas.
Using energy-efficient active or passive cooling systems and building designs in workplaces has numerous benefits. Cooling the environment is one of the most effective methods for reducing the risk of heat illness. Energy-efficient cooling reduces electricity consumption and greenhouse gas emissions compared to conventional systems. Energy-efficient buildings cost less to operate, allowing greater productivity at lower cost and reduced fossil fuel use and community air pollution. Energy-efficient cooling also decreases the amount of electricity on the grid at one time, reducing the chances of blackouts during extreme weather events.
We must develop a new approach to building standards – energy-efficient, worker-centric cooling – that integrates both worker health and energy-efficiency considerations. Existing building-centric approaches that blanket-cool entire buildings to the same fixed temperature are energy inefficient and can lead to overcooling of unoccupied areas and increased costs. The urgent need for energy-efficient worker-centric cooling standards is highlighted, for example, by the 300–900 million ft2 per quarter rate of U.S. warehouse space under construction, and a growing warehouse workforce, in recent years.
There is a gap in standards that address both civilian worker health and energy-efficient cooling simultaneously. The U.S. Green Building Council (USGBC) has incorporated a worker-centric approach in its Leadership in Energy and Environmental Design (LEED) certification program. This approach includes pilot credits for Prevention through Design (PtD), which aims to minimize risks to workers by integrating safety measures into building design and redesign. One such example is ensuring roof features, such as vegetated roofs and solar panel installations, are arranged to minimize hazards like falls for maintenance personnel. However, there are no specific PtD standards or LEED credits for energy-efficient cooling approaches that address worker heat hazards. For example, there are no specific standards that incorporate the proximity of indoor cool-down areas to hot work areas, targeted cooling of certain work areas, or mobile outdoor cooling stations that leverage solar and electrochemical technology.
Although there are several potential mechanisms of support for energy-efficient cooling infrastructure for commercial buildings and small businesses, there is no program to assist employers and small businesses in integrating these technologies into worker-centric cooling infrastructure designs. Under the Inflation Reduction Act of 2022 (IRA), tax deductions are available through Internal Revenue Code (IRC) 179D for building owners to install or retrofit equipment aimed at improving energy efficiency, including HVAC systems such as heat pumps and building envelope improvements to “heat-proof” or weatherize structures. However, tax credits may be difficult to access and may not provide a sufficient degree of immediate support for small business owners struggling with inflation costs. While the Biden-Harris Administration has also launched a $14 billion National Clean Investment Fund that will provide Environmental Protection Agency (EPA) grants to small businesses for deploying clean technology projects, there are no earmarked funds for workplace solutions focused on energy-efficient cooling or resilience to extreme heat events that integrate worker health considerations. Current U.S. Small Business Administration efforts focus primarily on supporting small businesses with disaster recovery rather than resilience.
Effective cross-agency coordination is needed to accomplish an energy-efficient cooling transformation in U.S. workplaces, support small businesses, and contribute to the Healthy People 2030 goal of reducing workplace deaths. Coordination among existing agencies and external partners to address gaps in energy-efficient cooling technology, worker-centric designs, and heat-specific PtD building approaches will support a healthier, more productive, and sustainable U.S. workforce.
Plan of Action
Transforming workplace infrastructure to support a healthy, productive, and sustainable U.S. workforce against extreme heat requires coordination across multiple federal agencies. This plan offers the first steps in developing a structure for coordination, defining the approach, developing a roadmap for future actions, and ultimately catalyzing and piloting innovations and implementing and evaluating solutions.
This plan is guided by the following principles:
- Workplace deaths, illnesses, and injuries from heat exposure are preventable.
- Work equity should be incorporated into decision-making, in alignment with the Justice40 Initiative, to ensure benefit for workers who are most likely to be exposed to dangerous workplace heat and who live and work in communities overburdened by pollution from energy inefficient infrastructure.
- Demand for solutions will be supported by co-benefits of energy-efficient workplace cooling (e.g., reduced workplace costs; increased productivity; reduced greenhouse gas emissions, in alignment with National Climate Task Force Goals and the Department of Energy (DOE) Better Buildings® Better Climate Challenge; and sustainable workplaces that are resilient to extreme events, in alignment with the Biden Administration’s Bipartisan Infrastructure Law).
- High-level sponsorship and clarity of roles are critical to catalyzing the necessary coordination across federal agencies and with public and private partners.
Following an executive order from the President, the Office of Management and Budget should convene a multiagency working group to develop a plan for coordination and to outline a roadmap toward an energy-efficient workplace cooling transformation for a healthy, productive, and sustainable workforce. The working group should:
Recommendation 1. Be chaired by an agency that has experience in convening multisectoral collaborations and advocating for equitable health outcomes, such as the Department of Health and Human Services (HHS) Office of Climate Change and Health Equity. The inclusion of representatives from the following agencies and offices should be considered:
- DOE (e.g., Office of Energy Efficiency and Renewable Energy, Office of State and Community Energy Programs, Office of Small and Disadvantaged Business Utilization)
- Centers for Disease Control (CDC) and its National Institute for Occupational Safety and Health (NIOSH) (e.g., Small Business Assistance Program, National Personal Protective Tech Lab, Division of Science Integration)
- EPA (e.g., Office of Research and Development, Office of Environmental Justice and External Civil Rights)
- U.S. Small Business Administration (SBA) (e.g., Small Business Innovation Research Program, Office of Disaster Recovery and Resilience)
- OSHA (e.g., Directorate of Standards and Guidance)
- National Oceanic and Atmospheric Administration (NOAA) (e.g., Climate Program Office)
- Internal Revenue Service (IRS)
- Bureau of Labor Statistics (BLS) (e.g., Office of Compensation and Working Conditions)
- White House Climate Policy Office
Recommendation 2. Define roles and develop a plan to enhance coordination with public and private partners in developing and evaluating evidence-based worker-centric cooling infrastructure technologies and building designs. Partners should include those that develop or promote voluntary standards and guidelines for:
- buildings (e.g., USGBC LEED Program PtD initiative; American Society of Heating, Refrigerating and Air-Conditioning Engineers [ASHRAE] energy efficiency standard 90.1, 2022 and thermal environment standard 55, 2023; and EnergyStar)
- worker health (e.g., American Conference of Governmental Industrial Hygienist (ACGIH) heat stress and American Industrial Hygiene Association thermal stress working groups)
- and business and labor representatives identified by the working group.
Recommendation 3. Establish a consensus definition of energy-efficient worker-centric cooling using a combination of established metrics, including:
- metrics for energy efficiency and
- metrics for human effects of heat that account for work characteristics such as ambient heat exposure, workload, and clothing.
Recommendation 4. Outline existing pathways to support an energy-efficient workplace cooling transformation, including:
- IRA tax deductions for building owner energy-efficient installation or retrofitting (IRA 13303; IRC 179D)
- National Clean Investment Fund grants through EPA to small businesses deploying clean technology projects
- SBA Office of Disaster Recovery & Resilience business loans,
- and assess gaps, alternative incentive mechanisms for businesses, and the landscape of private and foundation funders to inform Step 5.
Recommendation 5. Articulate follow-on initiatives and identify leaders and potential funding approaches to advance the roadmap of policies to accelerate, scale up, and evaluate equitable deployment, maintenance, and evaluation of worker-centric energy-efficient cooling infrastructure. Policies considerations include:
- Grant funding mechanisms for research, development, and pilot implementation and evaluation of worker-centric building designs and cooling technologies, such as those through the EPA’s National Clean Investment Fund, SBA/SBIR, or NIOSH’s crowdsourcing mechanisms similar to the Respirator Fit Challenge mechanism. Matching of federal and private and foundation funding should be considered to support rapid development, prototyping, and evaluation of promising worker-centric cooling infrastructure technology and building designs.
- Funding for ASHRAE, LEED, and DOE initiatives focused on incorporating worker considerations into standard development and energy code validation processes that ultimately inform local building codes.
- Funding for the IRS to develop and implement alternative incentive mechanisms that reduce barriers and address gaps in support for businesses interested in implementing energy-efficient workplace cooling infrastructure.
- Funding for DOE to:
- develop a centralized clearinghouse to disseminate information on federal programs, incentives, and mechanisms for financing energy-efficient cooling retrofits and upgrades for businesses, including small businesses (similar to H.R. 4092; 113th Congress for schools)
- support coordination of state energy offices with health and labor departments to conduct coordinated outreach on implementation of energy-efficient worker-centric cooling approaches and initiatives, with a focus on small businesses and those with disproportionately exposed workers
Funding for agencies to work together to develop and implement approaches to track progress toward an energy-efficient workplace cooling transformation by combining data sources.
Conclusion
Given the growing threat to U.S. workers and businesses posed by illness, death, and reduced work productivity from increasing heat exposure, it is imperative to catalyze an energy-efficient workplace cooling transformation. There is currently a unique and timely opportunity to build upon national clean energy, climate, and infrastructure commitments and goals to address gaps in energy-efficient worker-centric cooling technology and PtD building standards. The proposed plan will incorporate high-level support, provide infrastructure for coordination among government agencies and nongovernmental partners, define the approach, and lay the groundwork for stimulating innovations in promising worker-centric cooling technologies and designs. This plan will produce a roadmap for an energy-efficient workplace cooling transformation that will support businesses in establishing the infrastructure needed for existing and upcoming workplace heat prevention requirements. The approach will build upon existing occupational health equity initiatives to reduce the risk of heat health effects for workers disproportionately affected by heat and small businesses. This initiative will ensure a healthier, more productive, and sustainable workforce with minimal cost and a substantial potential return on investment.
This idea of merit originated from our Extreme Heat Ideas Challenge. Scientific and technical experts across disciplines worked with FAS to develop potential solutions in various realms: infrastructure and the built environment, workforce safety and development, public health, food security and resilience, emergency planning and response, and data indices. Review ideas to combat extreme heat here.
Under federal OSHA standards for employers, workplaces are currently only required to address workplace heat if it is causing or likely to cause death or serious harm to employees. This OSHA “General Duty Clause” requirement is insufficient, as workers experience negative effects from workplace heat exposure — ranging from heat illness to death. OSHA is in the process of developing a workplace heat standard that considers engineering controls, such as workplace cooling, along with other requirements related to worker breaks, training, and hydration. Workplace cooling is a proposed federal rule element and is already relevant for U.S. states with indoor workplace heat regulations. Energy-efficient workplace cooling infrastructure transitions do not happen overnight. Investment now is important for states with existing heat rules and to prepare for the future state and/or federal heat rules.
Home cooling only partially addresses extreme heat health risks because many working-age adults spend half of their waking hours during the workweek at work. Further, increased energy-efficiency in the industrial sector, which currently accounts for 30% of U.S. greenhouse emissions, can reduce pollution in surrounding communities and blackout risk during extreme weather events.
Existing incentives and grants (e.g., IRA tax deductions for building owner energy-efficient installation or retrofitting, such as IRA 13303; IRC 179D; National Clean Investment Fund grants through EPA to small businesses deploying clean technology projects; and SBA Office of Disaster Recovery and Resilience loans) do not explicitly incorporate worker-centric designs that achieve climate, energy-efficiency, and worker health goals simultaneously. Further, tax deductions and grant programs provide short- and medium-term financial support for energy-efficient workplace cooling transitions. Without a roadmap to address explicit coordination, simplification in processes, and accessibility of incentives, small business owners may be unable to take advantage of these incentives.
Examples of data sources that could be considered are:
- Records of businesses obtaining incentives, such as IRA tax deductions and National Clean Investment Fund EPA grants, for energy-efficient cooling
- Federal databases to track bills and policies that support or integrate worker-centric energy-efficient cooling strategies or building designs
- Rates of reported workplace cooling and heat illness by industry/occupation using existing national survey mechanisms such as data from relevant CDC Behavioral Risk Factor Surveillance System (BRFSS) modules and the BLS Survey of Occupational Injuries and Illnesses
- Worker heat deaths, for example through existing BLS Census of Fatal Occupational Injuries and NIOSH Fatality Assessment and Control Evaluation programs
A Comprehensive Strategy to Address Extreme Heat in Schools
Requiring children to attend school when classroom temperatures are high is unsafe and reduces learning; yet closing schools for extreme heat has wide-ranging consequences for learning, safety, food access, and social determinants of health. Children are vulnerable to heat, and schooling is compulsory in the U.S. Families rely on schools for food, childcare, and safety. In order to protect the health and well-being of the nation’s children, the federal government must facilitate efforts to collect the data required to drive extreme heat mitigation and adaptive capacity, invest in more resilient infrastructure, provide guidance on preparedness and response, and establish enforceable temperature thresholds. To do this, federal agencies can take action through three paths of mitigation: data collection and collaboration, set policy, and investments.
Challenge and Opportunity
Schools are on the forefront of heat-related disasters, and the impact extends beyond the hot days. Extreme heat threatens students’ health and academic achievement and causes rippling effects across the social determinants of health in terms of food access, caregiver employment, and future employment/income for students. Coordinated preparation is necessary to protect the health and well-being of children during extreme heat events.
School Infrastructure Failure
Many schools do not have adequate infrastructure to remain cool during extreme heat events. At the start of the 2023–2024 academic year, schools in multiple locations were already experiencing failure due to extreme heat and were closing or struggling to hold classes in sweltering classrooms. The Center for Climate Integrity identified a 39% increase from 1970 to 2025 in the number of school districts that will have more than 32 school days over 80°F (their temperature cutoff for needing air-conditioning to function). The Government Accountability Office found in 2020 that 41% of public school districts urgently need upgrades to HVAC systems in at least half of their buildings, totaling 36,000 buildings nationally. The National Center for Education Statistics’ (NCES) most recent survey of the Condition of America’s Public School Facilities (2012–2013 school year) found 30% of school buildings did not have adequate air-conditioning. The numbers correlate with the population of disadvantaged students: 34% of schools where at least 75% of students are eligible for free or reduced lunch, and only 25% of schools where less than 35% of students are eligible for free/reduced lunch. NCES’s School Pulse Panel, implemented to document schools’ response to COVID-19, is expanding to include other topics relevant to federal, state, and local decision-makers. The survey includes heat-adjacent questions on indoor air quality, air filtration, and HVAC upgrades, but does not currently document schools’ ability to respond to extreme heat. Schools that are not able to maintain cool temperatures during extreme heat events directly affect child health and safety, and have an upstream impact on health.
Impact on Child Health and Safety
When temperatures rise on school days, local districts must decide whether to remain open or close. Both decisions can affect children’s health and safety. If schools remain open, students may be exposed to uncomfortable and unsustainable high temperatures in rooms with inadequate ventilation. Teachers in New York State reported extreme temperatures up to 94℉ inside the classroom and children passing out during September 2023 heatwaves. Spending time in the schoolyard may only compound the problem. Unshaded playgrounds and asphalt quickly heat up and may be hotter than surrounding areas, with surface temperatures that can cause burns. Similar to neighborhood tree cover, shade on school playgrounds is correlated with income (more income, more shade), leading to a higher risk of heat exposure for low-income and historically marginalized students. Children are vulnerable to heat and may have trouble cooling down when their body temperatures rise. Returning to hot classrooms will not provide them with an opportunity to cool down.
If schools close, children who are unable to access school food may go hungry. Procedures exist to ensure the continuation of school food service during unanticipated school closures, but it is not clear how food service would function if the building is overheated during extreme heat events. In New York City, an assessment of public cooling centers identified that nearly half were in senior centers and not open to children. If schools do not have sufficient heat mitigation and are closed for heat, children from low-income households, who are at higher risk for food insecurity and less likely to have air conditioning at home, may be left hot and hungry.
While some state and local education departments have developed plans for responding to extreme heat on school days, the guidance, topics, and level of detail varies across states. Further, while the National Integrated Heat Health Information System (NIHHIS) and the Centers for Disease Control and Prevention (CDC) have identified children as an at-risk group during heat events, they do not offer specific information on how schools can prepare and respond. A comprehensive playbook that provides guidance on the many challenges schools may encounter during extreme heat, and how to keep children safe, would enhance schools’ ability to function.
Impact on Learning and Social Determinants of Health
The cumulative impact on learning, income, and equity is large. When schools remain open, heat reduces student learning (a 1% reduction in learning for each 1℉ increase across the year). When schools close, children lose learning time. The nation experienced the rippling effects of school closures during the COVID-19 pandemic, when extended closures impacted the achievement gap, projected future earnings, and caregiver employment, particularly for women. Even five days of closure for snow days in a school year has been seen to reduce learning. The projected increase in the number of districts that experience more than 32 school days a year over 80℉ suggests the impact of heat on learning could be substantial, whether it is from school closure or from learning in overheated classrooms.
The impact on learning disproportionately affects students in low-income districts, often correlated with race due to historic redlining, as these districts have fewer funds available for school improvement projects and are more likely to have school buildings that lack sufficient cooling mechanisms. These disproportionate impacts foster increasing academic and economic inequity between students in low- and high-income school districts.
Existing Response: Infrastructure
The federal government is aware of the infrastructure challenges and is funding green and gray infrastructure improvements through several programs. The Renew America’s Schools grants focus on funding infrastructure upgrades for K-12 schools. In the initial round of applications, need far exceeded available funds, with 236 Local Education Authorities submitting eligible requests totaling $1.62 billion. In response to the overwhelming need, the Department of Energy (DOE) more than doubled planned funding and awarded $178 million in grants. Through the American Rescue Plan, the Environmental Protection Agency (EPA) is providing technical assistance to help communities develop plans to develop cooling centers in schools. Through the Inflation Reduction Act, EPA is helping schools develop and implement Indoor Air Quality management plans, which include maintenance of acceptable temperatures, with an anticipated $32 million in grant funding over five years. Multiple public and private programs have supported projects to increase green space and tree cover on school grounds, including grants from the U.S. Department of Agriculture (USDA) Forest Service and California Department of Forestry and Fire Protection (CAL FIRE).
These programs are substantial, but also substantially less than the demonstrated need. Embedding heat considerations into future school infrastructure projects and integrating explicit consideration of heat into existing projects would enable all of the activities supported through these grants to mitigate the impact of extreme heat concurrently. A coordinated effort could increase the impact of these funds.
Existing Response: Temperature Standards
Though many states, school districts, or health departments maintain and enforce standards for minimum required temperatures in occupied buildings, relatively few have similar standards for maximum acceptable temperatures. The Occupational Safety and Health Administration (OSHA) recommends indoor temperatures stay between 68℉ and 76℉ and is currently developing a national standard for protecting workers during extreme heat. Occupational standards for maximum indoor temperature exist in Oregon (80℉), Minnesota (77℉ to 86℉), and California (80℉ outdoors; indoors pending). As public schools are institutions where adults work and children, an at-risk group, are required to be present, a national standard on acceptable indoor temperatures should be developed to protect children’s health and learning.
Plan of Action
Managing extreme heat in American public school systems requires urgent action. While education is primarily under the authority of the state governments, the mission of the federal government is to ensure educational excellence and equal access. Federal agencies can facilitate data collection and collaboration, set standards to maintain safety, provide guidelines for local education authorities to follow, and coordinate different actions at state level and act as a source of expertise for capacity building for state and local actors. Similar to the actions outlined in a recent memo on developing heat-resilient schools in California, the federal government should take preemptive action across the nation.
Collect Data and Collaborate. Federal agencies need to collaborate and collect data to better understand and drive mitigation efforts to prepare for extreme heat for schools.
- The U.S. Department of Education (ED) should join NIHHIS as a partnering agency to collaborate on heat preparation and mitigation strategies specifically for schools.
- The NCES should update a national inventory of school infrastructure to identify schools that will need upgrades or investments in infrastructure to mitigate heat based on climate prediction.
- ED should collaborate with EPA and/or National Oceanic and Atmospheric Administration (NOAA) to collect data about heat at indoor and outdoor school facilities so as to provide better guidance to schools and direct heat mitigation efforts (e.g., increasing shade or tree cover on playgrounds). Mechanisms for this could be through creating an optional reporting function of EPA’s School IAQ Assessment tool (see recommendation below), adding heat-related questions to NCES’s School Pulse Panel, or through NOAA heat-island mapping campaigns.
- EPA should update its School IAQ Assessment and App to include heat-related information. This could include a checklist or questions related to extreme heat, including both before heat events (HVAC status, shade cover on school building and playground, plans for hot days, options for water/cooling for overheated students, and indicators of heat stress), and heat assessments on days at high temperatures (indoor temperature in classrooms, hallways, cafeteria, gym, and outdoor temperatures on playgrounds [air and surfaces], blacktop, and shaded areas).
- NCES should add heat-related questions to the School Pulse Panel survey to aid heat-mitigation efforts in the same way the survey was used for COVID-19 mitigation. There are existing questions related to indoor air quality, ventilation, and the state of HVAC systems. Similar questions should be added to collect data on indoor and outdoor temperatures in locations where students spend school time (classrooms, lunch room, playground) during hot months, use of building-wide or local air conditioning or fans to maintain temperature, and availability of cooling spaces if the whole building does not have air-conditioning.
- ED should collaborate with state and local education authorities to collect data on school closures and absences during heat events to identify places where heat affects students’ ability to participate due to extreme heat and the reasons that students are absent during extreme heat events. Data on absences should be used to proactively target places where heat is having a larger impact on access to education.
Set Policy. In order to prepare for future extreme heat events, federal agencies can take the following actions to set policy to expand the adaptive capacity of schools to protect U.S. educational employees and students:
- Similar to required minimum indoor temperatures, OSHA should establish a standard that sets the maximum classroom indoor temperatures at which cooling action must be taken or classrooms must be closed. OSHA is already considering a heat standard for outdoor workers; OSHA can set standards for school employees that would also protect students learning in those conditions.
- The Federal Emergency Management Agency (FEMA) should define school infrastructure as failing on school days above 80℉ outdoor temperature in schools without air conditioning or indoor temperature above 80℉ in classrooms. FEMA can then apply mitigation measures if the school is determined to have infrastructure failure, including providing funding for infrastructure upgrades.
- FEMA and other agencies that assess and predict hazard risk should explicitly consider schools’ capability to remain open and keep children safe during extreme heat events as part of their assessments.
- ED and the Department of Health and Human Services (HHS) should develop guidelines to protect students’ health, well-being, and learning during extreme heat events and include them in the Emergency Planning section of schoolsafety.gov guidance. This could include an updated and easily accessed, searchable, and centralized library of federal and state resources specifically tailored to heat stress in schools such as California’s EnvironScreen and US Climate Resilience Toolkit. This can expand the capacity of local and state actors and provide ongoing access to updates support. This also sets the stage for state governments to share resources and collaborate.
- NIHHIS should add resources for schools in a “For Schools” drop-down section of the Planning and Preparing page on HEAT.gov.
- USDA should develop a federal process to serve food in alternative locations when school buildings are overheated during extreme heat events, similar to New York State’s summer waiver allowing food service in alternate locations during heat events.
Invest in Schools. In order to prepare for and plan for future extreme heat events, EPA, the Consumer Product Safety Commission (CPSC), USDA, and the Department of Energy (DOE) can take the following actions to launch mitigation measures to improve the resilience of schools and alleviate the impact of heat on student and employee health:
- Existing projects focused on school upgrades should integrate consideration of heat mitigation into their programs.
- The Renew America’s Schools Grants and EPA’s Indoor Air Quality project should ensure that infrastructure upgrades they support for K-12 schools will also meet the needs of increasing temperatures. These projects already contribute substantial funding to projects that could affect heat mitigation. Explicitly planning for and investing in heat mitigation as part of those upgrades could reduce the need for additional upgrades to address heat.
- The CPSC should update their Public Playground Safety Handbook to include a more comprehensive overview of designing thermally comfortable playgrounds. The National Program for Playground Safety developed a good example of this for the Standards Council of Canada with specific details about designing thermally safe playgrounds. Programs supporting schoolyard redesign projects should follow these guidelines.
- Substantial funding needs to be allocated to invest in infrastructure, cooling technologies, retrofits, landscape, and other adaptive strategies to prepare for extreme heat. There needs to be investments in researching how much funding is needed and how to allocate that funding equitably. Data collection proposed above will help determine the scale of the need.
- More funding should be made available through the Inflation Reduction Act to make schools prepared to operate during heat events as part of the tax credits and clean energy initiatives.
- More funding should be made available for green schoolyards to increase natural cooling. For example, the CAL FIRE Green Schoolyards grants to mitigate heat through tree planting programs should be funded nationally.
- The EPA’s American Rescue Plan funding should be expanded to renovate schools to function as cooling centers, and major funding should be provided to implement upgrades nationally.
Conclusion
Extreme heat is an urgent problem for schools. Opportunities exist across the federal government to protect our nation’s future by protecting our children. Federal agencies can best support state and local schools through three paths of mitigation: collect data and collaborate, set policy, and invest in schools.
This idea of merit originated from our Extreme Heat Ideas Challenge. Scientific and technical experts across disciplines worked with FAS to develop potential solutions in various realms: infrastructure and the built environment, workforce safety and development, public health, food security and resilience, emergency planning and response, and data indices. Review ideas to combat extreme heat here.
Several examples of potential legislation exist at the state level in Mississippi (classrooms must be air-conditioned for schools to be accredited), Connecticut (schools with air conditioners must maintain temperatures below 78ºF), Washington (schools must be “reasonably free of… excessive heat”), and Hawaii (classrooms must be a “temperature acceptable for student learning”) and a bill is being considered in New York (cooling action must be taken at 82ºF; classrooms can’t be occupied above 88ºF).
Adapting the Nation to Future Temperatures through Heat-Resilient Procurement
Extreme chronic and acute heat exposes millions of American lives to dangerous health risks and threatens our infrastructure. Yet there are many physical solutions available to mitigate the risk of heat to people and systems in our built environments. Despite clear evidence that heat exposure is a substantial challenge to human health, economic vitality, and the goals of the Justice40 initiative, very little has been done to galvanize viable markets for materials and technologies that can improve heat resilience.
In order to spur demand and send a strong signal for beneficial private sector innovation and scale, the federal government can lead by example to drive the market for products and services that build heat resilience. The General Services Administration (GSA) should require new and existing public structures (e.g. buildings and parking lots), products, supplies, and service procurement to meet minimum requirements for heat adaptation. These requirements could be adapted from existing green codes (e.g., ASHRAE 189.1 and IEA’s Annex 80) that recognize some of the non-energy benefits of heat-resilient materials and products, recognized supply chain vulnerabilities due to extreme heat (e.g. specialty crops, commodity crops, livestock, pharmaceutical precursors, etc.), and best practices for workplace protections (e.g. Fair Food Program).
Challenge and Opportunity
The federal government’s market-making potential is substantial – purchasing more than $630 billion in goods and services in FY2021 alone. The GSA owns and leases over 363 million square feet of space in 8,397 buildings in more than 2,200 communities nationwide. Updating procurement requirements and solicitations to promote passive cooling and heat resilience is relatively straightforward since GSA already maintains a database for green and sustainable building materials, systems, and services that could be amended, rather than creating a new parallel standard. Further, procurement standard changes are within the purview of a relatively small number of policy actors, compared to policies that incentivize voluntary uptake or require broad enforcement to be effective.
Even small increases in market demand, driven by policy, can significantly reduce first costs, product availability, and innovation. For example, requirements for solar reflective shingles on residential homes in Los Angeles City and County (a market of roughly 10 million people) reduced costs for high-end shingle products by two-thirds and saw the introduction of mid- and low-cost product lines throughout the country. Similarly, joint innovation around a commitment to incorporating cool pavements into Los Angeles and Phoenix road maintenance and preservation programs has driven global product innovation, improved durability and aesthetics, and more efficient application processes that benefit communities nationwide. GSA action on procurement would send a much stronger market signal to many more communities.
Heat-resilient procurement will also benefit rapidly developing federal policy to promote reduced heat risk. In January 2024, the Federal Emergency Management Agency announced that it would fund investments in net-zero energy reconstruction in areas under a federal disaster declaration. The provisions, which explicitly highlight investments in passive cooling, apply to Public Assistance, the agency’s largest grant program; the Hazard Mitigation Grant Program; and the Building Resilient Infrastructure and Communities grant program. Heat-resilient interventions can be a net benefit to net-zero priorities, keeping buildings cooler as temperatures rise without driving up energy consumption. Further, heat-resilience procurement standards aligns with the Office of Management and Budget’s climate-smart infrastructure investments memorandum (M-24-03), which calls for incorporation of current and future climate change risk in infrastructure investments and maximizing sustainability over the system’s service life.
The regulatory groundwork and technical language required for these recommendations are already in place. Several state and model codes already have requirements that could easily be adopted or referenced by a procurement standard. For example, California’s Title 24 includes requirements for cool roofs, green roofs, and other heat-adaptive interventions for a variety of climate zones. Similarly, ASHRAE Standard 189.1, the International Energy Conservation Code, ASHRAE Standard 90.1, and the LEED voluntary program include prescriptive urban heat island mitigation or passive cooling requirements for U.S. climate zones.
In November 2022, the Biden-Harris Administration proposed the Federal Supplier Climate Risks and Resilience Rule, which would require federal contractors receiving more than $7.5 million in annual contracts to publicly disclose their greenhouse gas emissions and climate-related financial risks and set science-based emissions reduction targets. Requiring heat resilience would further push markets toward adaptation.
Executive Order 14057 on catalyzing American clean energy industries and jobs through federal sustainability and the accompanying Federal Sustainability Plan would, in part, create a mandate and mechanism to update federal policies for sustainability, climate action, and resilience. The order includes “buy clean” provisions for low-carbon materials, with a goal of net-zero procurement by 2050, and a Net-Zero Emissions Procurement Federal Working Group and Buy Clean Task Force that is required to report semiannually on progress toward clean procurement. As heat-resilience interventions like cool surfaces can drive down energy consumption, they are aligned with net-zero priorities.
Plan of Action
A number of existing policy pathways and fora could be leveraged to develop, standardize, and include heat-resilience standards in procurement. To start, the GSA could amend its Facilities Standards for the Public Building Service (P100) for public facilities and infrastructure projects to incorporate heat resilience by adopting ASHRAE 189.1 and resilient cooling practices articulated in the International Energy Agency’s Annex 80. Supportive engagement with the Net-Zero Emissions Procurement Federal Working Group would leverage internal reporting requirements to advance heat adaptation. Further, the Environmental Protection Agency (EPA) could incorporate ASHRAE 189.1 performance requirements for highly solar-reflective and vegetated materials into Energy Star, allowing those products to be included in Green Procurement Compilation.
To ensure heat-resilient supplies and services, the Federal Acquisition Register (FAR) could be updated to include disclosures on how those products and services improve or reduce resilience to heat. Relevant disclosures include, but are not limited to, extreme heat’s risk to: service provision, such as unsafe working conditions; 2) supply chains and key commodity provisions; and 3) infrastructure operations, such as adequate cooling of data center facilities. The FAR already recognizes the risk of climate change in its proposed implementation of section 5(b)(i) of Executive Order 14030, Climate-Related Financial Risk, to require major federal suppliers to publicly disclose greenhouse gas emissions and climate-related financial risk and to set science-based reduction targets. GSA could also increase the use of life-cycle cost assessments over the lowest first-cost procurement to recognize the broader economic and societal benefits gained from investments in sustainable and resilient products and services.
Interagency efforts, stewarded by the Interagency Working Group on Extreme Heat, could accelerate standards for heat-resilient building codes as well as product and services procurement. For example, the National Institute of Standards and Technology (NIST) works on other climate-related building standards through the National Windstorm Impact Reduction Program (NWIRP) and the National Construction Safety Team (NCST) Act, which authorizes NIST to investigate extreme weather events on buildings and inform the improvement of codes for the built environment. Further, the U.S. Department of Housing and Urban Development (HUD) establishes construction and safety standards, and the Department of Energy (DOE) proposes energy-efficiency standards for manufactured homes, which account for approximately 10% of single-family houses constructed in the U.S. annually and could include heat-resilient technologies. The U.S. Department of Agriculture’s federal public food procurement system (including the National School Lunch Program, Emergency Food Assistance Program, and Commodity Supplemental Food Program) could take better stock of extreme heat’s risks to the federal government’s ability to affordably procure essential food products. Finally, in alignment with the Occupational Health and Safety Administration’s National Emphasis Program on Extreme Heat, agencies that contract with high-risk industries (e.g. agriculture, construction, manufacturing, firefighters, etc.) should ask for the latest data on workplace injuries and deaths during heat season (April to October) before awarding contracts and rate contractors on heat safety upon contract completion.
Federally supported construction standards and procurement requirements can also be applied at any level of government: national, state, tribal, local, or even school districts and incentivized through federal financing of these subnational efforts.
Non-Federal Stakeholders
This effort would greatly benefit from robust engagement with organizations outside of the public sector. National laboratories such as Lawrence Berkeley National Lab, Oak Ridge National Lab, National Renewable Energy Lab, and Pacific Northwest National Lab have deep technical experience to identify heat-resilient technologies. Organizations such as the Cool Roof Rating Council (which rates roofing and wall material surface properties) and the National Fenestration Rating Council are entry points to technical support from its industry members. Code experts such as the New Buildings Institute and Regulatory Assistance Project could identify and modify existing code language to match the needs of federal procurement. The American Public Health Association, Smart Surfaces Coalition, Institute for Policy Integrity, and others can support a broader social cost benefit to determine what performance levels to require in procurement standards.
This idea of merit originated from our Extreme Heat Ideas Challenge. Scientific and technical experts across disciplines worked with FAS to develop potential solutions in various realms: infrastructure and the built environment, workforce safety and development, public health, food security and resilience, emergency planning and response, and data indices. Review ideas to combat extreme heat here.
Cool surfaces are not a monolithic product category. They encompass a huge variety of roofing, wall, and building attachment products spanning commercial, residential, multi-family, institutional, and industrial use cases. In nearly all of those contexts, there is an available, economically viable first-cost option that would promote heat resilience rather than exacerbate heat exposure.
Heat-resilient or passive-cooling procurement standards may generate net positive impacts on the budget. Looking at life-cycle costs and benefits, studies have found that $1 invested in passive cooling measures returns between $1.50 and $15.20.
Beyond the federal budget, mandatory heat-resilience policies also yield substantial social and market benefits. When procurement and codes require heat resilience at a municipal level (as they have in Los Angeles, for example), the budget impact has been negligible but has resulted in dramatically lower first costs for heat-resilient options like advanced cool roof shingles. Similarly, adding questions about heat resilience to the required responses for service procurement is not an undue or onerous burden on potential federal contractors. Heat costs American workers and businesses over $100 billion per year in lost productivity and wages. Investments in the built environment may substantially reduce that existing burden, yielding more equitable outcomes in line with Justice40 (the wage impact is felt most acutely by outdoor, agricultural, and warehouse workers) and potentially more tax revenue.
Enhanced Household Air Conditioning Access Data for More Targeted Federal Support Against Extreme Heat
While access to cooling is the most protective factor against extreme heat events, the U.S. Census lacks granular, residential data to determine who has access to air conditioning (AC). The addition of a question about household access to working AC to the Census American Community Survey, a nationally representative survey on the social, economic, housing, and demographic characteristics of the population, would have life-saving impacts.
This is especially essential as the U.S. is experiencing more frequent and intense extreme heat events, and extreme heat now kills more people than all other weather-related hazards. Many vulnerable demographics — including people who are elderly, low-income, African-American, socially isolated, as well as those with preexisting health conditions— are exposed to high temperatures within their homes.
Better data on working AC infrastructure in American homes would improve how the federal government and its state and local partners target local social services and interventions, such as emergency responder deployment during high-heat events, as well as distribute federal assistance funds, such as the Weatherization Assistance Program (WAP), Low Income Home Energy Assistance Program (LIHEAP), and funding from the Inflation Reduction Act (IRA) along with the Bipartisan Infrastructure Law (BIL).
Challenge and Opportunity
In 2019, the U.S. Census Bureau acknowledged the danger of heat by issuing the Community Resilience Estimates (CRE) for Heat. The CRE for Heat is a measure that combines 10 questions from the existing American Community Survey questions. The questions ask about:
- Financial hardship
- Older residents living alone
- Crowding
- Whether the home is a mobile home, boat, or recreational vehicle
- Employment status for those under 65 years old
- Whether a resident has a disability
- Whether a resident has health insurance
- Access to a vehicle
- Connection via broadband internet access
- Communication barriers
However, the CRE for Heat lacks a question about air conditioning, the most important protective factor. Indoor temperature regulation is essential for mitigating heat illness and death on extremely hot days – temperatures above 86°F indoors can easily become dangerous and deadly.
Currently, the best information on residential AC is provided by the biennial American Housing Survey (AHS). In 2019, the AHS reported that 8.8% (11.6 million households) of all U.S. housing units have no form of AC. However, this information has three significant weaknesses. First, the American Housing Survey is based on 2,000 homes sampled across a metropolitan area. The sampling process generates an average across high-, medium-, and low-income residents; therefore, it overestimates the presence of AC in lower-income households. American households with higher incomes are more likely to have access to AC: 92.2% of households with incomes greater than $100,000 have some form of AC, compared with 88.9% of households with incomes less than $30,000. Second, lower-income households may have broken AC systems or units and lack money for repairs, skewing collected data. Third, the AHS fails to consider how poverty constrains electricity consumption. Many lower-income households reduce or abstain from using their AC in fear of costly electricity bills that trigger shutoffs. For instance, a 2022 report found that nearly 20% of households earning less than $25,000 reported keeping their indoor temperatures at levels that felt unsafe for several months of the year. These three weaknesses of the AHS data underscore the need for fine-grained information on who has access to working AC, especially in lower-income households.
The U.S. Census American Community Survey (ACS), on the other hand, samples 3.5 million addresses every year in a nationally representative annual survey. The ACS asks about housing characteristics, costs, and conditions (including heating) but not about AC nationwide. The equivalent survey administered in the four Island Areas of Guam, the Commonwealth of the Northern Mariana Islands, the U.S. Virgin Islands, and American Samoa — known as the “Island Areas Census” — included an AC question until 2010. This is an important precedent for adding a similar question to all Census surveys and should expedite the process. However, adding the term “working” (or a similar word) to the air-conditioning question would enhance its ability to capture low-income homes with broken systems as well as households that cannot use their existing AC due to energy insecurity.
Former question on air-conditioning in the American Community Survey for U.S. Island Areas
Better Information for Better Distribution of LIHEAP and WAP Funding
In addition to helping emergency responders, city planners, and public health departments, information collected on the presence of working AC could help ensure that the Department of Health and Human Services (HHS) Low Income Heat Energy Assistance Program (LIHEAP) and Department of Energy’s (DOE) Weatherization Assistance Program (WAP) serve the most vulnerable residents.
LIHEAP, administered by the Office of Community Services (OCS) within the Administration for Children and Families (ACF), is designed to “assist low-income households, particularly those in the lowest incomes, that pay a high proportion of household income for home energy, primarily in meeting their home energy needs.” LIHEAP is a targeted block grant program whereby states distribute their funds across three programs that subsidize home energy heating or cooling costs; fund payment in crises; and support home weatherization (limited to 15% of funds unless a state requests a waiver to increase their percentage to 25%). The largest proportion of the funds subsidizes lower-income, vulnerable residents’ energy spending. While LIHEAP is an important federal program that impacted 7.1 million American households in 2023, only approximately 20% of eligible households received LIHEAP assistance, and the program is currently facing budget shortfalls of $2 billion.
By expanding cooling assistance, LIHEAP is being asked to do more with less: 24 of 50 states now include cooling assistance, and 9.8% of funds subsidized cooling costs. As extreme heat events become more frequent and severe and households become more energy insecure in the face of rising energy prices, more states will need to expand cooling assistance programs. Data on where households are most vulnerable — that is, those households without working AC or the financial ability to operate their AC — would enable targeted distribution of federal funds. Therefore, adding a Census question on household access to working AC would provide critical information to ensure LIHEAP funds serve the most vulnerable households.
Unlike LIHEAP, WAP’s sole focus is weatherization. Many weatherization improvements that help in cold weather also improve indoor thermal comfort during warm summer months. These improvements include fixing broken AC; adding insulation in walls, attics, and crawlspaces; and replacing leaky, inoperable windows. Compared to LIHEAP, WAP serves a much smaller number of homes — 35,000 homes annually versus LIHEAP’s 7.1 million (as of FY2023). Knowing the number of individual households in a census tract in need of investments in heat resilience adaptation and air-conditioning would enable much more targeted delivery of limited federal resources. Further, DOE can use this information to predict future grid demand and enhance necessary resilience measures for hotter summers.
Plan of Action
To save lives in the face of growing extreme heat, the Census should add a question about working AC to the American Community Survey. This could be executed as follows:
Recommendation 1. The Office of Community Services in the Administration for Children and Families (OCS ACF) requests the addition of a question about access to working AC at the census tract level to the American Community Survey. This would directly aid the LIHEAP program’s mandate to identify and serve vulnerable individuals, and benefit other programs like DOE’s WAP as well as programs authorized by the IRA and BIL.
Recommendation 2. Legal staff in the Office of Management and Budget (OMB) and the Census Bureau review the proposal to determine whether it meets legislative requirements.
Recommendation 3. After a successful legal review, OMB and the Census Bureau, in consultation with the Interagency Council on Statistical Policy Subcommittee for the American Community Survey, determine whether the request merits consideration.
Recommendation 4. Subject matter experts across relevant federal government programs (i.e. LIHEAP and WAP) and external institutions (housing experts, extreme heat experts, social vulnerability experts) identify ways to ask the question. The Census Bureau conducts interviews to determine which wording produces the most accurate results. Because a similar question (but lacking the term “working”) is used on the American Community Survey for Island Areas, this process may be expedited. A potential example of the new question is below:
Do you have working air air-conditioning?
- Yes, a central air conditioning system (includes split-type)
- Yes, 1 individual room unit
- Yes, 2 or more individual room units
- No, my air conditioning system is non-functional or broken
- No, I cannot afford to run my air-conditioning system
- No, I do not have any air-conditioning system
Recommendation 5. The Census Bureau solicits public comment on the question and request OMB’s approval for field testing.
Recommendation 6. The Census Bureau and ACF OCS review the results and decide whether to recommend adding the new survey question. Through the Federal Register Notice, the Census Bureau solicits public comment. Public comments inform the final decision that is made in consultation with the OMB and the Interagency Council on Statistical Policy Subcommittee on the American Community Survey.
Recommendation 7. If approved by OMB, the Census Bureau adds the question to its materials, and implementation begins at the start of the following calendar year (October).
Recommendation 8. The Community Resilience Estimates (CRE) for Heat is updated with information about AC as it becomes available. This tool can be shared, along with refined guidance, with state-level administrators of programs like LIHEAP and WAP to target investments to the households most vulnerable to overheating and resulting heat illness and death. The CDC could integrate AC coverage within its existing syndromic surveillance programs on extreme heat, as an additional layer of “risk” for targeted public health deployment during high-heat events.
Conclusion
The U.S. lacks fine-scaled data to determine whether households can access working AC systems/units and operate them during extreme heat events. Adding a question to the American Community Survey will provide life-saving information for emergency responders, social service providers, and city staff as extreme heat events become more frequent and intense. This fine-scaled information will also aid in distributing LIHEAP and WAP funding and increase the federal government’s ability to protect the most vulnerable residents from life-threatening extreme heat events.
This idea of merit originated from our Extreme Heat Ideas Challenge. Scientific and technical experts across disciplines worked with FAS to develop potential solutions in various realms: infrastructure and the built environment, workforce safety and development, public health, food security and resilience, emergency planning and response, and data indices. Review ideas to combat extreme heat here.
Combating Extreme Heat with a National Moonshot
Extreme heat is the leading cause of weather-related deaths in the United States and has been for the past 30 years. Low-income communities and many other vulnerable populations are disproportionately affected by heat risk. As the climate continues to warm, the threat to public health will correspondingly increase. Through a presidential directive, the White House Climate Policy Office (WHCPO) should establish the National Moonshot to Combat Extreme Heat, an all-of-government program to harmonize and accelerate federal efforts to reduce heat risk and heat illness, save lives, and improve the cost-effectiveness of federal expenditures.
The goals of the Moonshot are to:
- Reduce heat deaths by 20% by 2030, 40% by 2035, and 60% by 2050.
- Build 150 heat-resilient communities by 2030 by facilitating access to funding and uplifting social infrastructure actions prioritizing at-risk, vulnerable populations.
- Increase visibility and awareness of federal efforts to protect residents from extreme heat.
The Moonshot will be overseen by a new, high-level appointee at WHCPO to serve as the Executive Officer of the White House Interagency Work Group on Extreme Heat (WHIWG).
Challenge and Opportunity
The threat to public health and safety from extreme heat is serious, expansive, and increasing as the planet continues to warm. According to Heat.gov, “Extreme heat has been the greatest weather-related cause of death in the U.S. for the past 30 years — more than hurricanes, tornadoes, flooding or extreme cold.” The number of deaths from extreme heat is difficult to accurately determine and is frequently undercounted. More recently, during the Heat Dome of 2021, the state of Washington reported 1,231 heat deaths in just one month. Further, heat-related illness includes a broad spectrum of diseases, from mild heat cramps to life-threatening heat stroke. Heat exposures have been linked to mental health illnesses and adverse birth outcomes, such as preterm births and low birth weights. Extreme heat disproportionately impacts marginalized people, including those that are low-income, BIPOC, seniors, veterans, children, the unhoused, and those with compromised health status, among others. All heat illnesses and deaths are considered preventable.
Extreme heat is an all-of-society problem that requires an all-of-government response. As the frequency, intensity, duration, and breadth of heat waves have increased dramatically over the past four years, officials and leaders at all levels have begun taking action.
The federal government has launched new programs for addressing extreme heat over the last few years as heat waves have become a front-page issue. Recent programs initiated by the Biden Administration are providing a variety of resources and increasing awareness of this threat. Key examples are:
- The White House Interagency Work Group on Extreme Heat (WHIWG) on Extreme Heat was launched in September 2021 to coordinate a “holistic” response. The WHIWG began work with the National Integrated Heat Health Information System (NIHHIS) to develop a National Heat Strategy in July 2023. Information about the WHIWG is primarily communicated to the public through press releases from the White House. The initiative announced several new actions to address heat, including a rulemaking process at the Occupational Safety and Health Administration (OSHA) to develop a workplace heat standard and actions and ongoing data collection efforts (i.e., syndromic surveillance and heat island mapping campaigns) by the Centers for Disease Control and Prevention (CDC) and NIHHIS. The White House also announced a new set of planning tools to address extreme heat in April 2023 as part of the American Rescue Plan.
- In addition to working with the WHIWG, NIHHIS collaborates with the CDC and over 20 other federal agencies through Heat.gov, a resource hub for federal extreme heat and health information. NIHHIS focuses on developing and sharing information and tools, increasing interagency coordination, and developing a National Heat Strategy.
- The National Climate Resilience (NCR) Framework takes a high-level approach to building climate resilience through six overarching objectives. However, detailed treatment of extreme heat in the Framework is minimal.
Actions are needed to remedy the deficit in attention to extreme heat by uplifting the role of extreme heat in the federal response to climate impacts and give greater emphasis to social infrastructure actions.
Several bills to address extreme heat through federal legislation have been introduced in Congress, though none have advanced. Most notable are:
- S. 2645: Senator Edward Markey’s Preventing HEAT Illness and Deaths Act of 2023 would authorize NIHHIS to prescribe actions and provide funding.
- HR 3965: Representative Ruben Gallego’s “Extreme Heat Emergency Act of 2023” would amend the Stafford Act by adding “extreme heat” as a natural disaster for which response aid is authorized.
- H.R. 2945: Representative Ruben Gallego’s Excess Urban Heat Mitigation Act of 2023” would require the Department of Housing and Urban Development (HUD) to establish a grant program to fund activities to mitigate or manage heat in urban areas. The Senate version of this bill, S. 1379, is led by Senator Sherrod Brown.
Even with this momentum, actions are dispersed across many departments and agencies. Plus, many local and state governments tend to apply for federal funding on a program-by-program, agency-by-agency basis and must navigate a complicated landscape with limited funding explicitly earmarked for heat resilience. Further, most “infrastructure” and capacity-building funding is based on mitigating or restoring economic loss of property, leading to financial relief that has gone primarily to built infrastructure and natural infrastructure projects. Communities need social infrastructure: social cohesion, policy and governance, public health, communications and alerts, planning, etc., to respond to extreme heat. This requires a pathway for communities to access funds to combat extreme heat in a comprehensive and coordinated way and bring social infrastructure actions up to a level equal to built and natural infrastructure interventions.
There is a need to improve the coordination of heat actions across the federal government, align heat resilience activities with Justice40 mandates, and promote community-based interventions to reduce heat deaths. A National Moonshot to Combat Extreme Heat can do this by leveraging several new community-focused programs to accelerate the protection of at-risk populations from heat-related death and illness. The challenge, and therefore the opportunity, for the Moonshot is to identify, integrate, and accelerate existing resources in a human-centric framework to reduce preventable deaths, promote cool and healthy communities, and deliver value nationwide.
Plan of Action
The WHCPO should appoint a new Deputy Director for Heat to serve as the Executive Officer of the WHIWG and coordinate the National Moonshot to Combat Extreme Heat – an all-of-government program to accelerate federal actions to address extreme heat. The goals of the Moonshot are to:
- Reduce heat deaths by 20% by 2030, 40% by 2035, and 60% by 2050;
- Build 150 heat-resilient communities by 2030 by facilitating access to funding and uplifting social infrastructure actions prioritizing at-risk, vulnerable populations. Social infrastructure encompasses a variety of actions in four categories: social cohesion, policy, communications, and planning. Social infrastructure centers the needs of people in resilience. This target aligns with the U.S. goal to reduce greenhouse gas emissions by 50% by 2030.
- Improve visibility and awareness of federal efforts to protect residents from extreme heat.
The Moonshot will capitalize on existing policies, programs, and funding and establish a human-centric approach to climate resilience by uplifting extreme heat. The Moonshot will identify and evaluate existing federal activities and available funding, including funds from the Inflation Reduction Act (IRA) and the Bipartisan Infrastructure Law (BIL), as well as agency budgets, including Federal Emergency Management Agency’s funding for the Building Resilient Infrastructure and Communities (BRIC) and the Hazard Mitigation Grant Program (HMGP). The Moonshot will integrate actions among the many existing programs dispersed across the government into a well-coordinated, integrated inter-agency initiative that maximizes results and will support cool, safe, and healthy communities
Recommendation 1. Enhance the visibility, responsibility, and capacity of the WHIWG.
Signaling high-level support through a presidential directive, the WHCPO should appoint a Deputy Director for Heat as the Executive Officer of the WHIWG to lead the Moonshot. Two additional staff positions will be established to support the assessment, stakeholder engagement, and planning processes. The WHIWG and the Deputy Director will design and implement the Moonshot working with the Department of Health and Human Services Office of Climate Change and Health Equity. A lead contact will be designated in each agency and department participating in the NIHHIS program.
Recommendation 2. Assess and report current status.
The Moonshot should identify, evaluate, and report on existing programs addressing heat across the federal government, including those recently launched by the White House, to establish a current baseline, identify gaps, and catalog opportunities for integration within the federal government. The Moonshot will generate a database of existing programs and a budget cross-cut analysis to identify current funding levels. The report will incorporate the NIHHIS Extreme Heat Strategy and identify existing funding opportunities, including those in the IRA, Bipartisan Infrastructure Law, and agency programs. The Moonshot will also work with CDC and NIHHIS to develop a method to identify heat deaths to establish a baseline for tracking progress on the goals.
Recommendation 3. Build broad community support.
The Moonshot should convene conversations and conduct regional extreme heat workshops with state, local, and tribal government personnel; external experts and stakeholders; Justice40 community leaders; professional associations; private sector representatives; and philanthropies. Topics should span the spectrum of social infrastructure, including social cohesion, public health, insurance, infrastructure, communications, and more. Based on input, the Moonshot will establish an advisory committee of non-government participants and develop pathways to connect stakeholders with federal community-focused climate resilience programs, including the White House’s Justice 40 program, EPA’s Environmental Justice Thriving Communities Technical Assistance Centers Program, and the Department of Transportation’s Thriving Communities Network, and other relevant federal programs identified in Recommendation 2. The Moonshot would add extreme heat as a covered issue area in these programs.
Recommendation 4. Make a plan.
The Moonshot should expand upon the NIHHIS Extreme Heat Strategy and make a heat action plan uplifting human health and community access to harness the potential of federal heat programs. The plan would assign roles, responsibilities, and deadlines and establish a process to track and report progress annually. In addition, the Moonshot would expand the NCR Framework to include an implementation plan and establish a human-centric approach. The Moonshot will evaluate co-benefits from heat reduction strategies, including the role cool surfaces play in protecting public health while also decreasing smog, reducing energy use, and solar radiation management. And, consistent with the Biden Administration’s 2025 priorities, the Moonshot will support research and development on emerging technologies such as microfiber fabrics that keep people cool during heat waves, temperature-sensitive coatings, and high-albedo reflective materials that can reduce the need for mechanical air-conditioning. Innovation is especially needed related to resurfacing the nation’s aging roadways.
The Moonshot will also include a communications plan to increase awareness of federal programs and funding opportunities to combat extreme heat. This should all be in place in nine months to prepare for the FY 2026 budget. The NIHHIS and CDC will develop an enhanced method for improving the accuracy of tracking heat deaths.
Recommendation 5. Connect with people and communities.
The Moonshot should emphasize social infrastructure projects and facilitate access to funding by establishing a centralized portal for comprehensive local heat action planning and programs. The Moonshot will help build cool, safe, healthy communities by integrating heat into federal climate equity programs and supporting local heat plans and projects that reflect community input and priorities. Local heat plans should be comprehensive and integrate a suite of actions that emphasize social infrastructure and include built infrastructure and natural infrastructure.
Recommendation 6. Initiate all-of-government action.
The Moonshot will catalyze the implementation of the plan across the government, including all the agencies and departments identified in Recommendation 1. It will establish the grant portal to enhance access to federal resources for heat-related projects for state, local, tribal, and territorial governments, and community groups. It will launch a communications plan targeting press, social media, public employees at all levels of government, stakeholders, and more.
Recommendation 7. Support legislation to secure long-term success
In coordination with the White House Office of Legislative Affairs and Office of Management and Budget (OMB), the Moonshot should work with Congress to draft and support federal legislation and appropriations addressing extreme heat. Congressional authority is needed to firmly establish this human-centric approach to extreme heat. The Moonshot may recommend Congressional hearings on legislation or a Congressional commission to review the Administration’s work on heat. For example, the passage of S. 2645 would enshrine the position of NIHHIS in law. The Moonshot will help Congress fulfill its role in the all-of-government response and help empower local action.
Costs
Using information gathered in Recommendation 2, the Moonshot will focus on capturing and directing existing federal funding, including from the IRA, BIL, agency budgets, and grant programs to uplift actions addressing extreme heat and implementing the Moonshot action plan. Initial costs should be minimal: $1 million to hire the Executive Director and two staff and to report on existing programs, funding, and agency budgets. The Moonshot will produce a budget cross-cut initially and annually thereafter and assemble a budget proposal for the WHIWG on Extreme Heat for the FY 2025 and FY 2026 budget.
The Moonshot recommendation is aligned with the OMB Budget Memo of August 17, 2023, which transmits Guidance for Research and Development Priorities for the FY 2025 Budget. The OMB priorities call for addressing climate change by protecting communities’ health and mitigating its health effects, especially for communities that experience these burdens disproportionately.
Conclusion
Extreme heat is a serious public health problem disproportionately impacting many vulnerable populations, and the threat is increasing tremendously. So far in winter 2023, more than 130 monthly high-temperature records were set across the U.S.
The federal government has several programs addressing the threat of extreme heat in the U.S., and the WHIWG reflects the all-of-government approach needed to meet the threat. The next step is to capture the full potential of existing programs and funding by launching a focused and intensive National Moonshot to Combat Extreme Heat with quantitative goals to track and reduce heat deaths and build healthy communities. This effort will enable state and local governments and communities, especially those disproportionately impacted by extreme heat, to more readily access federal funding to develop and implement comprehensive heat action plans. The Moonshot will reduce heat deaths, improve the quality of life in cities, and reduce economic productivity loss while increasing the visibility of federal leadership on this issue.
With heat season 2024 beginning on April 29th, it’s essential to establish an all-of-government response to address extreme heat at all levels.
This idea of merit originated from our Extreme Heat Ideas Challenge. Scientific and technical experts across disciplines worked with FAS to develop potential solutions in various realms: infrastructure and the built environment, workforce safety and development, public health, food security and resilience, emergency planning and response, and data indices. Review ideas to combat extreme heat here.
Federal agencies involved in NIHHIS include: National Oceanic and Atmospheric Administration, Centers for Disease Control and Prevention, Administration for Community Living, Administration for Children and Families, Administration for Strategic Preparedness and Response, Environmental Protection Agency, Department of Housing and Urban Development, Federal Emergency Management Agency, Department of Defense, Department of Energy, Department of Transportation, National Institute for Occupational Safety and Health, Department of Veterans Affairs, US Census Bureau, Forest Service, National Park Service, Department of Health and Human Services, National Institute of Environmental Health Sciences, Occupational Safety and Health Administration, Substance Abuse and Mental Health Services Administration, and United States Agency for International Development.
Non-federal partners include, but are not limited to: CAPA Strategies, ESRI, Global Cool Cities Alliance, National League of Cities, and Global Heat Health Information Network.
Adopting Evidence-Based Heat Stress Management Strategies In The Workplace
Millions of workers are subjected to the dangers of extreme heat that increase their risk of heat-related illnesses and fatalities. Due to personal, social, and workplace vulnerabilities, workers are at even greater risk, particularly women, people who are Black or Brown, those who facing low-income challenges, and those employed by small businesses. With no mandated federal heat stress standard, there is no federal mechanism to ensure the adoption of appropriate heat stress prevention strategies and emergency procedures to protect vulnerable workers.
Now is an opportune time to introduce a federal program to champion climate equity and justice in the workplace by assisting employers’ implementation of evidence-based heat stress management strategies and heat illness emergency procedures, particularly targeting underserved working populations who labor in the heat. This program should be supported by the Occupational Safety and Health Administration (OSHA), along with university and nonprofit partners, and funded through a private or public partnership. This effort will act on the principles of employer social responsibility, best practice recognition, increased resource allocation to vulnerable working groups, third-party auditing, and a non-retaliation reporting mechanism. This policy action, across multiple stakeholders, will proactively address the challenges posed by extreme heat and work toward creating safer, more equitable working environments for all.
Challenge and Opportunity
The average global surface temperature in 2023 was 2.12ºF above the 20th century average, resulting in Earth’s warmest year on record. Extreme temperatures will continue to rise as the frequency, intensity, and duration of heat waves increase due to climate change. Climate change is a major public health priority that places workers who perform physical labor in the heat at higher risk, due to frequent prolonged, heavy physical exertion, layers of personal protective clothing, and exposure to environmental heat stress. This combination of factors exacerbates the level of heat stress placed on the body, leading to heat-related injuries, illnesses, and fatalities. While the Biden Administration has initiated federal action to establish a mandated heat standard, the bureaucratic process is slow, averaging around eight years. Congress is also working on addressing this issue through the consideration of a bill for the adoption of an emergency temporary standard. Although it offers a quicker solution, it has a limited life span of approximately six months. Moreover, in anticipation of mandating a federal heat stress standard, there is limited infrastructure to support the adoption of evidence-based heat stress management strategies to protect workers in high-temperature environments. The current enforcement solution, OSHA’s National Emphasis Program on outdoor and indoor heat hazards, has several limitations, include such as a vague definition of noncompliant following heat hazard inspection, and uses assessment tools such as Heat Index, which is not considered “best practice.”
To address these limitations, key stakeholders from academic settings, large research institutes, and nonprofit organizations have developed evidence-based best practices to protect vulnerable workers from extreme heat. Unfortunately, there is no system in place to determine how well companies are prepared for extreme heat. The urgency of adopting evidence-based heat stress management strategies across industries cannot be overstated, as heat-related injuries and fatalities are entirely preventable with the implementation of appropriate prevention strategies and emergency procedures.
There is a critical opportunity to champion climate equity and justice to safeguard laborers from the dangers of extreme heat. Laborers from vulnerable demographics who engage in physical work in the heat are disproportionately affected and are often not protected under evidence-based heat stress management practices by their employers. Workers with personal (e.g., age, race/ethnicity, disease status) and social (e.g., employment type, income status) vulnerabilities are exploited by working in hot environments with limited heat stress prevention strategies available to them. This form of labor exploitation during periods of high heat exposure leaves millions of U.S. workers more vulnerable to preventable heat-related injuries and fatalities.
Small businesses and other companies with limited resources are also less equipped to protect their workforce or have the means to ensure their employees are working in safe environments in the heat. To fortify workplace resilience against extreme heat and climate change, it is imperative to equitably distribute resources for enforcing evidence-based heat policies in workplaces. Organizations with employees exposed to high temperatures must be held accountable for the effective implementation of these policies. Additionally, vulnerable workers frequently refrain from reporting unsafe conditions due to the fear of employer retaliation. Advocacy efforts become even more challenging as language barriers, food insecurity, and poverty exacerbate already dire working conditions.
The present moment presents an opportune time to introduce a program supported by occupational health and safety federal agencies. As evidence-based best practices have been developed to protect workers from extreme heat, there is no system in place to protect vulnerable working populations, allocate resources, and keep companies accountable by assessing their current heat stress management practices. OSHA and the National Institute for Occupational Safety and Health (NIOSH) are key stakeholder organizations to initiate a federal response to address the lack of adoption of heat stress management policies. However, these entities often prioritize multiple projects simultaneously, are understaffed, and benefit from partnerships with universities and nonprofits. Therefore, a cooperative approach with governing like OSHA and universities/nonprofit organizations is the appropriate strategy to create a program that promotes the enforcement of evidence-based heat protection strategies (i.e., education, hydration, heat acclimatization, environmental monitoring, physiological monitoring) at the organizational level. This approach also provides under-resourced businesses with access to basic heat protection equipment and establishes a mechanism for employees to report unsafe working conditions without fear of retaliation. This program draws inspiration from the success of the Fair Food Program, a Corporate Social Responsibility model that promotes accountability among growers, buyers, and retailers.
This comprehensive program will support all organizations that employ workers who perform physical work in the heat, such as construction, utilities, agriculture, oil, and gas. This program will facilitate employer accountability, social responsibility, increased resource allocation, third-party auditing, and a non-retaliation reporting system.
Plan of Action
The development and implementation of this federal program, the Occupational Heat Resiliency Program (OHRP), will require a public-private partnership between OSHA, universities, and nonprofit partners. This partnership model draws inspiration from the successful collaborative partnerships between OSHA and other partners to protect the workforce against other occupational hazards. The OHRP will promote the adoption of evidence-based heat stress management practices by targeting employers with workplaces that experience high heat exposure and/or have a large population of laborers working in the heat who are classified as vulnerable workers. The establishment of OHRP will require funding through cooperative agreements, such as the OSHA Strategic Partnership Program (OSPP). To achieve the program’s objectives, both OSHA and its partners will commit their knowledge and resources to support the program.
The program will rely on the following principles to achieve this objective:
- Employer accountability and best practice recognition:
- Employers engaging with the proposed federal program will formalize their commitment to safeguarding workers from extreme heat through evidence-based practices derived from original research from research institutes and academic organizations. These original research sources have informed governing body recommendations from institutes such as NIOSH.
- These commitments can be publicized, creating transparency and ensuring that products are manufactured by adequately protected workers.
- The program aims to promote the adoption of evidence-based heat practices that enhance safety, health, and productivity for the U.S. workforce.
- Recognition of best practices will facilitate widespread adoption, empowering employers, safety professionals, and workers to implement strategies and emergency procedures that effectively mitigate the risk of heat-related illnesses and injuries.
- Climate equity through increased resource allocation:
- Recognizing the disproportionate impact of climate change on vulnerable populations, the program will allocate resources to workplaces with high percentages (>50%) of at-risk workers. This includes small businesses and workplaces with a high percentage of women, people of Color, and low-income workers. Workplace needs will be performed through existing efforts related to other occupational hazards or community projects and by targeting industries associated with increased employment of vulnerable workers.
- Support may include assistance in creating heat stress management educational materials and emergency action plans/procedures, implementing written heat stress management plans, and providing essential resources such as hydration, shade, and cooling products.
- Safer work environments through third-party auditing and a non-retaliation reporting system:
- Third-party audits, led by university or non-profit partners, will determine feasible evidence-based practices and resource allocations.
- Audits will employ a tier system (I, II, II) to show the level of protection that the workplace has implemented based on the presented recommendations. To ensure compliance, a non-retaliation reporting system will allow workers to report incidences where their work environment was unsafe due to extreme heat.
- A non-retaliation reporting system will be implemented to empower workers to report unsafe conditions due to extreme heat, ensuring employer compliance and accountability. This information within the report will not be shared with employers directly, but rather through the third-party auditing entity.
The program will be led by teams composed of OSHA representatives and university/nonprofit partners that will meet virtually regularly to ensure the goals of each principle are being met and to address any partnership issues that may arise.
Conclusion
The escalating challenges to the U.S. workforce posed by extreme heat demand proactive measures, necessitating collaboration among key government entities like OSHA alongside universities and nonprofit organizations. Currently, there is a glaring absence of mechanisms to safeguard workers who engage in physical work in the heat, particularly those from vulnerable demographics.
To tackle this issue head-on, the establishment of OHRP funded through a private or public partnership is imperative. This initiative would champion climate equity in the workplace by expediting the adoption of evidence-based heat stress management strategies and emergency procedures. The program’s framework includes commitments from employers, recognition of best practices, increased resource allocation to vulnerable working groups, third-party auditing, and a non-retaliation mechanism. OHRP will have an immediate impact at both the federal and state level. Without the implementation of such a program, a significant portion of the U.S. workforce remains at risk of entirely preventable heat-related injuries, illnesses, and fatalities.
This idea of merit originated from our Extreme Heat Ideas Challenge. Scientific and technical experts across disciplines worked with FAS to develop potential solutions in various realms: infrastructure and the built environment, workforce safety and development, public health, food security and resilience, emergency planning and response, and data indices. Review ideas to combat extreme heat here.
The program will require approximately $10 million for its initial three-year phase for startup, launch, and execution. A three-year projection is a conservative time based on the time frame for launching similar federal programs. The budget will be allocated to two areas:
- Time, labor, and travel costs for program management (~$8 million)
- Resource allocation for vulnerable working groups (i.e., small businesses, businesses with a high percentage of low-income workers) (~$2 million)
Following the three-year phase, approximately $1-2 million per year will be needed to reach more vulnerable working populations.