U.S. Energy Security Compacts: Enhancing American Leadership and Influence with Global Energy Investment
This policy proposal was incubated at the Energy for Growth Hub and workshopped at FAS in May 2024.
Increasingly, U.S. national security priorities depend heavily on bolstering the energy security of key allies, including developing and emerging economies. But U.S. capacity to deliver this investment is hamstrung by critical gaps in approach, capability, and tools.
The new administration should work with Congress to give the Millennium Challenge Corporation (MCC) the mandate and capacity to lead the U.S. interagency in implementing ‘Energy Security Compacts’, bilateral packages of investment and support for allies whose energy security is closely tied to core U.S. priorities. This would require minor amendments to the Millennium Challenge Act of 2003 to add a fourth business line to MCC’s Compact operations and grant the agency authority to coordinate an interagency working group contributing complementary tools and resources.
This proposal presents an opportunity to deliver on global energy security, an issue with broad appeal and major national security benefits. This initiative would strengthen economic partnerships with allies overseas, who consistently rank energy security as a top priority; enhance U.S. influence and credibility in advancing global infrastructure; and expand growing markets for U.S. energy technology. This proposal is built on the foundations and successes of MCC, a signature achievement of the G.W. Bush administration, and is informed by lessons learned from other initiatives launched by previous presidents of both parties.
Challenge and Opportunity
More than ever before, U.S. national security depends on bolstering the energy security of key allies. Core examples include:
- Securing physical energy assets: In countries under immediate or potential military threat, the U.S. may seek to secure vulnerable critical energy infrastructure, restore energy services to local populations, and build a foundation for long-term restoration.
- Countering dependence on geostrategic competitors: U.S. allies’ reliance on geostrategic competitors for energy supply or technologies poses short- and long-term threats to national security. Russia is building large nuclear reactors in major economies including Turkey, Egypt, India, and Bangladesh; has signed agreements to supply nuclear technology to at least 40 countries; and has agreed to provide training and technical assistance to at least another 14. Targeted U.S. support, investment, and commercial diplomacy can head off such dependence by expanding competition.
- Driving economic growth and enduring diplomatic relationships: Many developing and emerging economies face severe challenges in providing reliable, affordable electricity to their populations. This hampers basic livelihoods; constrains economic activity, job creation, and internet access; and contributes to deteriorating economic conditions driving instability and unrest. Of all the constraints analyses conducted by MCC since its creation, roughly half identified energy as a country’s top economic constraint. As emerging economies grow, their economic stability has an expanding influence over global economic performance and security. In coming decades, they will require vast increases in reliable energy to grow their manufacturing and service industries and employ rapidly growing populations. U.S. investment can provide the foundation for market-driven growth and enduring diplomatic partnerships.
- Diversifying supply chains: Many crucial technologies depend on minerals sourced from developing economies without reliable electricity. For example, Zambia accounts for about 4% of global copper supply and would like to scale up production. But recurring droughts have shuttered the country’s major hydropower plant and led to electricity outages, making it difficult for mining operations to continue or grow. Scaling up the mining and processing of key minerals in developing economies will require investment in improving power supply.
The U.S. needs a mechanism that enables quick, efficient, and effective investment and policy responses to the specific concerns facing key allies. Currently, U.S. capacity to deliver such support is hamstrung by key gaps in approach, capabilities, and tools. The most salient challenges include:
A project-by-project approach limits systemic impact: U.S. overseas investment agencies including the Development Finance Corporation (DFC), the U.S. Trade and Development Agency (USTDA), and the Export-Import Bank (EXIM) are built to advance individual commercial energy transactions across many different countries. This approach has value–but is insufficient in cases where the goal is to secure a particular country’s entire energy system by building strong, competitive markets. That will require approaching the energy sector as a complex and interconnected system, rather than a set of stand-alone transactions.
Diffusion of tools across the interagency hinders coordination. The U.S. has powerful tools to support energy security–including through direct investment, policy support, and technical and commercial assistance–but they are spread across at least nine different agencies. Optimizing deployment will require efficient coordination, incentives for collaboration; and less fragmented engagement with private partners.
Insufficient leverage to incentivize reforms weakens accountability. Ultimately, energy security depends heavily on decisions made by the partner country’s government. In many cases, governments need to make tough decisions and advance key reforms before the U.S. can help crowd in private capital. Many U.S. agencies provide technical assistance to strengthen policy and regulatory frameworks but lack concrete mechanisms to incentivize these reforms or make U.S. funding contingent on progress.
Limited tools supporting vital enabling public infrastructure blocks out private investment. The most challenging bottleneck to modernizing and strengthening a power sector is often not financing new power generation (which can easily attract private investment under the right conditions), but supporting critical enabling infrastructure including grid networks. In most emerging markets, these are public assets, wholly or partially state-owned. However, most U.S. energy finance tools are designed to support only private sector-led investments. This effectively limits their effectiveness to the generation sector, which already attracts far more capital than transmission or distribution.
To succeed, an energy security investment mechanism should:
- Enable investment highly tailored to the specific needs and priorities of partners;
- Provide support across the entire energy sector value chain, strengthening markets to enable greater direct investment by DFC and the private sector;
- Co-invest with partner countries in shared priorities, with strong accountability mechanisms.
Plan of Action
The new administration should work with Congress to give the Millennium Challenge Corporation the mandate to implement ‘Energy Security Compacts’ (ESCs) addressing the primary constraints to energy security in specific countries, and to coordinate the rest of the interagency in contributing relevant tools and resources. This proposal builds on and reflects key lessons learned from previous efforts by administrations of both parties.
Each Energy Security Compact would include the following:
- A process led by MCC and the National Security Council (NSC) to identify priority countries.
- An analysis jointly conducted by MCC and the partner country on the key constraints to energy security.
- Negotiation, led by MCC with support from NSC, of a multi-year Energy Security Compact, anchored by MCC support for a specific set of investments and reforms, and complemented by relevant contributions from the interagency. The Energy Security Compact would define agency-specific responsibilities and include clear objectives and measurable targets.
- Implementation of the Energy Security Compact, led by MCC and NSC. To manage this process, MCC and NSC would co-lead an Interagency Working Group comprising representatives from all relevant agencies.
- Results reporting, based on MCC’s top-ranked reporting process, to the National Security Council and Congress.
This would require the following congressional actions:
- Amend the Millennium Challenge Act of 2003: Grant MCC the expanded mandate to deploy Energy Security Compacts as a fourth business line. This should include language applying more flexible eligibility criteria to ESCs, and broadening the set of countries in which MCC can operate when implementing an ESC. Give MCC the mandate to co-lead an interagency working group with NSC.
- Plus up MCC Appropriation: ESCs can be launched as a pilot project in a few markets. But ultimately, the model’s success and impact will depend on MCC appropriations, including for direct investment and dedicated staff. MCC has a track record of outstanding transparency in evaluating its programs and reporting results.
- Strengthen DFC through reauthorization. The ultimate success of ESCs hinges on DFC’s ability to deploy more capital in the energy sector. DFC’s congressional authorization expires in September 2025, presenting an opportunity to enhance the agency’s reach and impact in energy security. Key recommendations for reauthorization include: 1) Addressing the equity scoring challenge; and 2) Raising DFC’s maximum contingent liability to $100 billion.
- Budget. The initiative could operate under various budget scenarios. The model is specifically designed to be scalable, based on the number of countries with which the U.S. wants to engage. It prioritizes efficiency by drawing on existing appropriations and authorities, by focusing U.S. resources on the highest priority countries and challenges, and by better coordinating the deployment of various U.S. tools.
This proposal draws heavily on the successes and struggles of initiatives from previous administrations of both parties. The most important lessons include:
- From MCC: The Compact model works. Multi-year Compact agreements are an effective way to ensure country buy-in, leadership, and accountability through the joint negotiation process and the establishment of clear goals and metrics. Compacts are also an effective mechanism to support hard infrastructure because they provide multi-year resources.
- From MCC: Investments should be based on rigorous analysis. MCC’s Constraints Analyses identify the most important constraints to economic growth in a given country. That same rigor should be applied to energy security, ensuring that U.S. investments target the highest impact projects, including those with the greatest positive impact on crowding in additional private sector capital.
- From Power Africa: Interagency coordination can work. Coordinating implementation across U.S. agencies is a chronic challenge. But it is essential to ESCs–and to successful energy investment more broadly. The ESC proposal draws on lessons learned from the Power Africa Coordinator’s Office. Specifically, joint-leadership with the NSC focuses effort and ensures alignment with broader strategic priorities. A mechanism to easily transfer funds from the Coordinator’s Office to other agencies incentivizes collaboration, and enables the U.S. to respond more quickly to unanticipated needs. And finally, staffing the office with individuals seconded from relevant agencies ensures that staff understand the available tools, how they can be deployed effectively, and how (and with whom) to work with to ensure success. Legislative language creating a Coordinator’s Office for ESCs can be modeled on language in the Electrify Africa Act of 2015, which created Power Africa’s interagency working group.
Conclusion
The new administration should work with Congress to empower the Millennium Challenge Corporation to lead the U.S. interagency in crafting ‘Energy Security Compacts’. This effort would provide the U.S. with the capability to coordinate direct investment in the energy security of a partner country and contribute to U.S. national priorities including diversifying energy supply chains, investing in the economic stability and performance of rapidly growing markets, and supporting allies with energy systems under direct threat.
This action-ready policy memo is part of Day One 2025 — our effort to bring forward bold policy ideas, grounded in science and evidence, that can tackle the country’s biggest challenges and bring us closer to the prosperous, equitable and safe future that we all hope for whoever takes office in 2025 and beyond.
PLEASE NOTE (February 2025): Since publication several government websites have been taken offline. We apologize for any broken links to once accessible public data.
MCC’s model already includes multi-year Compacts targeting major constraints to economic growth. The agency already has the structure and skills to implement Energy Security Compacts in place, including a strong track record of successful investment across many energy sector compacts. MCC enjoys a strong bipartisan reputation and consistently ranks as the world’s most transparent bilateral development donor. Finally, MCC is unique among U.S. agencies in being able to put large-scale grant capital into public infrastructure, a crucial tool for energy sector support–particularly in emerging and developing economies. Co-leading the design and implementation of ESCs with the NSC will ensure that MCC’s technical skills and experience are balanced with NSC’s view on strategic and diplomatic goals.
This proposal supports existing proposed legislative changes to increase MCC’s impact by expanding the set of countries eligible for support. The Millennium Challenge Act of 2003 currently defines the candidate country pool in a way that MCC has determined prevents it from “considering numerous middle-income countries that face substantial threats to their economic development paths and ability to reduce poverty.” Expanding that country pool would increase the potential for impact. Secondly, the country selection process for ESCs should be amended to include strategic considerations and to enable participation by the NSC.
Mobilizing Innovative Financial Mechanisms for Extreme Heat Adaptation Solutions in Developing Nations
Global heat deaths are projected to increase by 370% if direct action is not taken to limit the effects of climate change. The dire implications of rising global temperatures extend across a spectrum of risks, from health crises exacerbated by heat stress, malnutrition, and disease, to economic disparities that disproportionately affect vulnerable communities in the U.S. and in low- and middle-income countries. In light of these challenges, it is imperative to prioritize a coordinated effort at both national and international levels to enhance resilience to extreme heat. This effort must focus on developing and implementing comprehensive strategies to ensure the vulnerable developing countries facing the worst and disproportionate effects of climate change have the proper capacity for adaptation, as wealthier, developed nations mitigate their contributions to climate change.
To address these challenges, the U.S. Agency for International Development (USAID) should mobilize finance through environmental impact bonds focused on scaling extreme heat adaptation solutions. USAID should build upon the success of the SERVIR joint initiative and expand it to include a partnership with NIHHIS to co-develop decision support tools for extreme heat. Additionally, the Bureau for Resilience, Environment, and Food Security (REFS) within the USAID should take the lead in tracking and reporting on climate adaptation funding data. This effort will enhance transparency and ensure that adaptation and mitigation efforts are effectively prioritized. By addressing the urgent need for comprehensive adaptation strategies, we can mitigate the impacts of climate change, increase resilience through adaptation, and protect the most vulnerable communities from the increasing threats posed by extreme heat.
Challenge
Over the past 13 months, temperatures have hit record highs, with much of the world having just experienced their warmest June on record. Berkeley Earth predicts a 95% chance that 2024 will rank as the warmest year in history. Extreme heat drives interconnected impacts across multiple risk areas including: public health; food insecurity; health care system costs; climate migration and the growing transmission of life-threatening diseases.
Thus, as global temperatures continue to rise, resilience to extreme heat becomes a crucial element of climate change adaptation, necessitating a strategic federal response on both domestic and international scales.
Inequitable Economic and Health Impacts
Despite contributing least to global greenhouse gas emissions, low- and middle-income countries experience four times higher economic losses from excess heat relative to wealthier counterparts. The countries likely to suffer the most are those with the most humidity, i.e. tropical nations in the Global South. Two-thirds of global exposure to extreme heat occurs in urban areas in the Global South, where there are fewer resources to mitigate and adapt.
The health impacts associated with increased global extreme heat events are severe, with projections of up to 250,000 additional deaths annually between 2030 and 2050 due to heat stress, alongside malnutrition, malaria, and diarrheal diseases. The direct cost to the health sector could reach $4 billion per year, with 80% of the cost being shouldered by Sub-Saharan Africa. On the whole, low-and middle-income countries (LMICs) in the Global South experience a higher portion of adverse health effects from increasing climate variability despite their minimal contributions to global greenhouse emissions, underscoring a clear global inequity challenge.
This imbalance points to a crucial need for a focus on extreme heat in climate change adaptation efforts and the overall importance of international solidarity in bolstering adaptation capabilities in developing nations. It is more cost-effective to prepare localities for extreme heat now than to deal with the impacts later. However, most communities do not have comprehensive heat resilience strategies or effective early warning systems due to the lack of resources and the necessary data for risk assessment and management — reflected by the fact that only around 16% of global climate financing needs are being met, with far less still flowing to the Global South. Recent analysis from Climate Policy Initiative, an international climate policy research organization, shows that the global adaptation funding gap is widening, as developing countries are projected to require $212 billion per year for climate adaptation through 2030. The needs will only increase without direct policy action.
Opportunity: The Role of USAID in Climate Adaptation and Resilience
As the primary federal agency responsible for helping partner countries adapt to and build resilience against climate change, USAID announced multiple commitments at COP28 to advance climate adaptation efforts in developing nations. In December 2023, following COP28, Special Presidential Envoy for Climate John Kerry and USAID Administrator Power announced that 31 companies and partners have responded to the President’s Emergency Plan for Adaptation and Resilience (PREPARE) Call to Action and committed $2.3 billion in additional adaptation finance. Per the State Department’s December 2023 Progress Report on President Biden’s Climate Finance Pledge, this funding level puts agencies on track to reach President Biden’s pledge of working with Congress to raise adaptation finance to $3 billion per year by 2024 as part of PREPARE.
USAID’s Bureau for Resilience, Environment, and Food Security (REFS) leads the implementation of PREPARE. USAID’s entire adaptation portfolio was designed to contribute to PREPARE and align with the Action Plan released in September 2022 by the Biden Administration. USAID has further committed to better integrating adaptation in its Climate Strategy for 2022 to 2030 and established a target to support 500 million people’s adaptation efforts.
This strategy is complemented by USAID’s efforts to spearhead international action on extreme heat at the federal level, with the launch of its Global Sprint of Action on Extreme Heat in March 2024. This program started with the inaugural Global Heat Summit and ran through June 2024, calling on national and local governments, organizations, companies, universities, and youth leaders to take action to help prepare the world for extreme heat, alongside USAID Missions, IFRC and its 191-member National Societies. The executive branch was also advised to utilize the Guidance on Extreme Heat for Federal Agencies Operating Overseas and United States Government Implementing Partners.
On the whole, the USAID approach to climate change adaptation is aimed at predicting, preparing for, and mitigating the impacts of climate change in partner countries. The two main components of USAID’s approach to adaptation include climate risk management and climate information services. Climate risk management involves a “light-touch, staff-led process” for assessing, addressing, and adaptively managing climate risks in non-emergency development funding. The climate information services translate data, statistical analyses, and quantitative outputs into information and knowledge to support decision-making processes. Some climate information services include early warning systems, which are designed to enable governments’ early and effective action. A primary example of a tool for USAID’s climate information services efforts is the SERVIR program, a joint development initiative in partnership with the National Aeronautics and Space Administration (NASA) to provide satellite meteorology information and science to partner countries.
Additionally, as the flagship finance initiative under PREPARE, the State Department and USAID, in collaboration with the U.S. Development Finance Corporation (DFC), have opened an Adaptation Finance Window under the Climate Finance for Development Accelerator (CFDA), which aims to de-risk the development and scaling of companies and investment vehicles that mobilize private finance for climate adaptation.
Plan of Action
Recommendation 1: Mobilize private capital through results-based financing such as environmental impact bonds
Results-based financing (RBF) has long been a key component of USAID’s development aid strategy, offering innovative ways to mobilize finance by linking payments to specific outcomes. In recent years, Environmental Impact Bonds (EIBs) have emerged as a promising addition to the RBF toolkit and would greatly benefit as a mechanism for USAID to mobilize and scale novel climate adaptation. Thus, in alignment with the PREPARE plan, USAID should launch an EIB pilot focused on extreme heat through the Climate Finance for Development Accelerator (CFDA), a $250 million initiative designed to mobilize $2.5 billion in public and private climate investments by 2030. An EIB piloted through the CFDA can help unlock public and private climate financing that focuses on extreme heat adaptation solutions, which are sorely needed.
With this EIB pilot, the private sector, governments, and philanthropic investors raise the upfront capital and repayment is contingent on the project’s success in meeting predefined goals. By distributing financial risk among stakeholders in the private sector, government, and philanthropy, EIBs encourage investment in pioneering projects that might struggle to attract traditional funding due to their novel or unproven nature. This approach can effectively mobilize the necessary resources to drive climate adaptation solutions.
This approach can effectively mobilize the necessary resources to drive climate adaptation solutions.
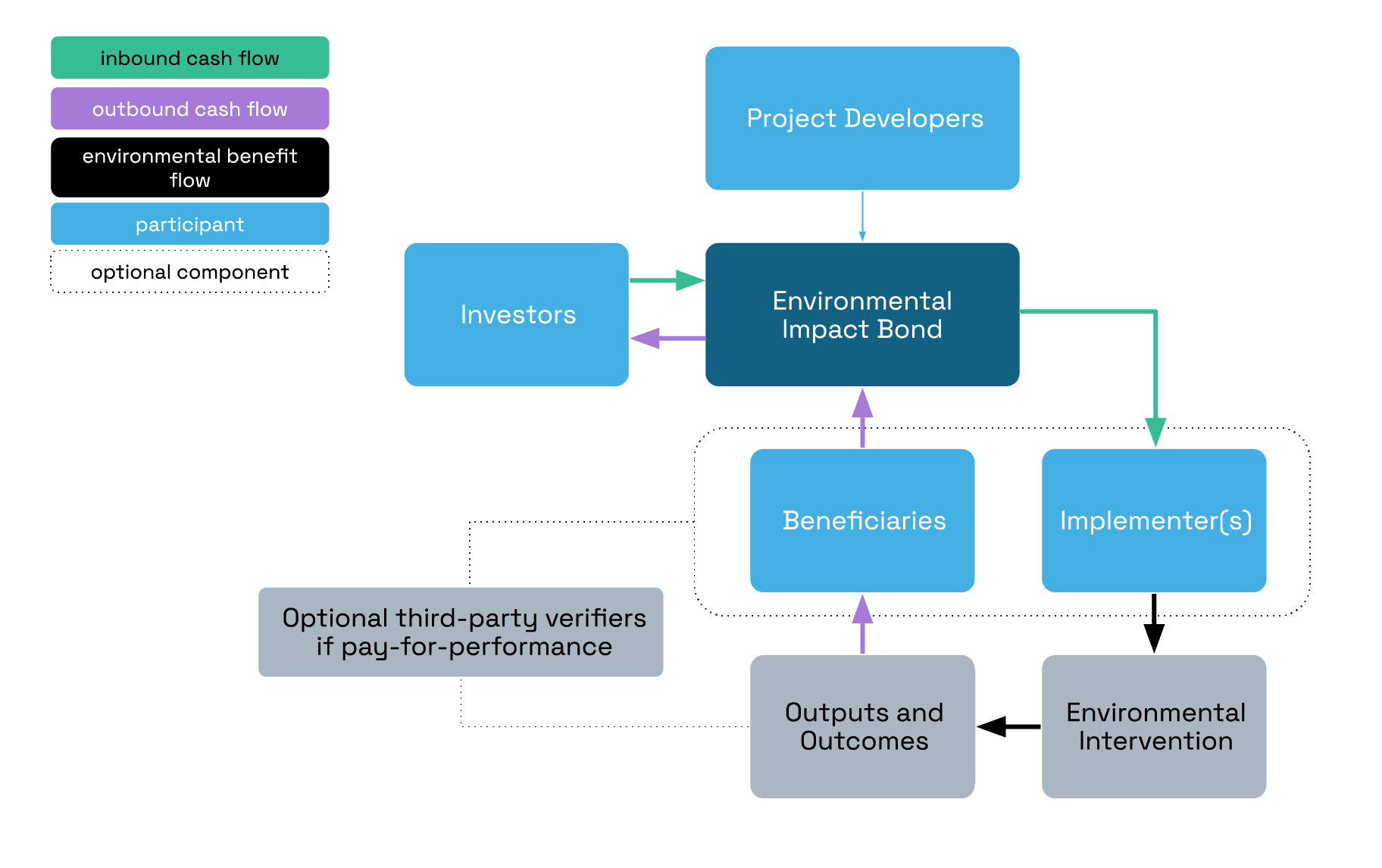
Overview of EIB structure, including cash flow (purple and green arrows) and environmental benefits (black arrows).
Adapted from Environmental Impact Bonds: a common framework and looking ahead
The USAID EIB pilot should focus on scaling projects that facilitate uptake and adoption of affordable and sustainable cooling systems such as solar-reflective roofing and other passive cooling strategies. In Southeast Asia alone, annual heat-related mortality is projected to increase by 295% by 2030. Lack of access to affordable and sustainable cooling mechanisms in the wake of record-shattering heat waves affects public health, food and supply chain, and local economies. An EIB that aims to fund and scale solar-reflective roofing (cool roofs) has the potential to generate high impact for the local population by lowering indoor temperature, reducing energy use for air conditioning, and mitigating the heat island effect in surrounding areas. Indonesia, which is home to 46.5 million people at high risk from a lack of access to cooling, has seen notable success in deploying cool roofs/solar-reflective roofing through the Million Cool Roof Challenge, an initiative of the Clean Cooling Collaborative. The country is now planning to scale production capacity of cool roofs and set up its first testing facility for solar-reflective materials to ensure quality and performance. Given Indonesia’s capacity and readiness, an EIB to scale cool roofs in Indonesia can be a force multiplier to see this cooling mechanism reach millions and spur new manufacturing and installation jobs for the local economy.
To mainstream EIBs and other innovative financial instruments, it is essential to pilot and explore more EIB projects. Cool roofs are an ideal candidate for scaling through an EIB due to their proven effectiveness as a climate adaptation solution, their numerous co-benefits, and the relative ease with which their environmental impacts can be measured (such as indoor temperature reductions, energy savings, and heat island index improvements). Establishing an EIB can be complex and time-consuming, but the potential rewards make the effort worthwhile if executed effectively. Though not exhaustive, the following steps are crucial to setting up an environmental impact bond:
Analyze ecosystem readiness
Before launching an environmental impact bond, it’s crucial to conduct an analysis to better understand what capacities already exist among the private and public sectors in a given country to implement something like an EIB. Additionally working with local civil society organizations is important to ensure climate adaptation projects and solutions are centered around the local community.
Determine the financial arrangement, scope, and risk sharing structure
Determine the financial structure of the bond, including the bond amount, interest rate, and maturity date. Establish a mechanism to manage the funds raised through the bond issuance.
Co-develop standardized, scientifically verified impact metrics and reporting mechanism
Develop a robust system for measuring and reporting the environmental impact projects; With key stakeholders and partner countries, define key performance indicators (KPIs) to track and report progress.
USAID has already begun to incubate and pilot innovative financing mechanisms in the global health space through development impact bonds. The Utkrisht Impact Bond, for example, is the world’s first maternal and newborn health impact bond, which aims to reach up to 600,000 pregnant women and newborns in Rajasthan, India. Expanding the use case of this financing mechanism in the climate adaptation sector can further leverage private capital to address critical environmental challenges, drive scalable solutions, and enhance the resilience of vulnerable communities to climate impacts.
Recommendation 2: USAID should expand the SERVIR joint initiative to include a partnership with NIHHIS and co-develop decision support tools such as an intersectional vulnerability map.
Building on the momentum of Administrator Power’s recent announcement at COP28, USAID should expand the SERVIR joint initiative to include a partnership with NOAA, specifically with NIHHIS, the National Integrated Heat Health Information System. NIHHIS is an integrated information system supporting equitable heat resilience, which is an important area that SERVIR should begin to explore. Expanded partnerships could begin with a pilot to map regional extreme heat vulnerability in select Southeast Asian countries. This kind of tool can aid in informing local decision makers about the risks of extreme heat that have many cascading effects on food systems, health, and infrastructure.
Intersectional vulnerabilities related to extreme heat refer to the compounding impacts of various social, economic, and environmental factors on specific groups or individuals. Understanding these intersecting vulnerabilities is crucial for developing effective strategies to address the disproportionate impacts of extreme heat. Some of these intersections include age, income/socioeconomic status, race/ethnicity, gender, and occupation. USAID should partner with NIHHIS to develop an intersectional vulnerability map that can help improve decision-making related to extreme heat. Exploring the intersectionality of extreme heat vulnerabilities is critical to improving local decision-making and helping tailor interventions and policies to where it is most needed. The intersection between extreme heat and health, for example, is an area that is under-analyzed, and work in this area will contribute to expanding the evidence base.
The pilot can be modeled after the SERVIR-Mekong program, which produced 21 decision support tools throughout the span of the program from 2014-2022. The SERVIR-Mekong program led to the training of more than 1,500 people, the mobilization of $500,000 of investment in climate resilience activities, and the adoption of policies to improve climate resilience in the region. In developing these tools, engaging and co-producing with the local community will be essential.
Recommendation 3: USAID REFS and the State Department Office of Foreign Assistance should work together to develop a mechanism to consistently track and report climate funding flow. This also requires USAID and the State Department to develop clear guidelines on the U.S. approach to adaptation tracking and determination of adaptation components.
Enhancing analytical and data collection capabilities is vital for crafting effective and informed responses to the challenges posed by extreme heat. To this end, USAID REFS, along with the State Department Office of Foreign Assistance, should co-develop a mechanism to consistently track and report climate funding flow. Currently, both USAID and the State Department do not consistently report funding data on direct and indirect climate adaptation foreign assistance. As the Department of State is required to report on its climate finance contributions annually for the Organisation for Economic Co-operation and Development (OECD) and biennially for the United Nations Framework Convention on Climate Change (UNFCCC), the two agencies should report on adaptation funding at similarly set, regular interval and make this information accessible to the executive branch and the general public. A robust tracking mechanism can better inform and aid agency officials in prioritizing adaptation assistance and ensuring the US fulfills its commitments and pledges to support global adaptation to climate change.
The State Department Office of Foreign Assistance (State F) is responsible for establishing standard program structures, definitions, and performance indicators, along with collecting and reporting allocation data on State and USAID programs. Within the framework of these definitions and beyond, there is a lack of clear definitions in terms of which foreign assistance projects may qualify as climate projects versus development projects and which qualify as both. Many adaptation projects are better understood on a continuum of adaptation and development activities. As such, this tracking mechanism should be standardized via a taxonomy of definitions for adaptation solutions.
Therefore, State F should create standardized mechanisms for climate-related foreign assistance programs to differentiate and determine the interlinkages between adaptation and mitigation action from the outset in planning, finance, and implementation — and thereby enhance co-benefits. State F relies on the technical expertise of bureaus, such as REFS, and the technical offices within them, to evaluate whether or not operating units have appropriately attributed funding that supports key issues, including indirect climate adaptation.
Further, announced at COP26, PREPARE is considered the largest U.S. commitment in history to support adaptation to climate change in developing nations. The Biden Administration has committed to using PREPARE to “respond to partner countries’ priorities, strengthen cooperation with other donors, integrate climate risk considerations into multilateral efforts, and strive to mobilize significant private sector capital for adaptation.” Co-led by USAID and the U.S. Department of State (State Department), the implementation of PREPARE also involves the Treasury, NOAA, and the U.S. International Development Finance Corporation (DFC). Other U.S. agencies, such as USDA, DOE, HHS, DOI, Department of Homeland Security, EPA, FEMA, U.S. Forest Service, Millennium Challenge Corporation, NASA, and U.S. Trade and Development Agency, will respond to the adaptation priorities identified by countries in National Adaptation Plans (NAPs) and nationally determined contributions (NDCs), among others.
As USAID’s REFS leads the implementation of the PREPARE and hosts USAID’s Chief Climate Officer, this office should be responsible for ensuring the agency’s efforts to effectively track and consistently report climate funding data. The two REFS Centers that should lead the implementation of these efforts include the Center for Climate-Positive Development, which advises USAID leadership and supports the implementation of USAID’s Climate Strategy, and the Center for Resilience, which supports efforts to help reduce recurrent crises — such as climate change-induced extreme weather events — through the promotion of risk management and resilience in the USAID’s strategies and programming.
In making standardized processes to prioritize and track the flow of adaptation funds, USAID will be able to more effectively determine its progress towards addressing global climate hazards like extreme heat, while enhancing its ability to deliver innovative finance and private capital mechanisms in alignment with PREPARE. Additionally, standardization will enable both the public and private sectors to understand the possible areas of investment and direct their flows for relevant projects.
USAID uses the Standardized Program Structure and Definitions (SPSD) system — established by State F — to provide a common language to describe climate change adaptation and resilience programs and therefore enable the comparison and analysis of budget and performance data within a country, regionally or globally. The SPSD system uses the following categories: (1) democracy, human rights, and governance; (2) economic growth; (3) education and social services; (4) health; (5) humanitarian assistance; (6) peace and security; and (7) program development and oversight. Since 2016, climate change has been in the economic growth category and each climate change pillar has separate Program Areas and Elements. The SPSD consists of definitions for foreign assistance programs, providing a common language to describe programs. By utilizing a common language, information for various types of programs can be aggregated within a country, regionally, or globally, allowing for the comparison and analysis of budget and performance data.
Using the SPSD program areas and key issues, USAID categorizes and tracks the funding for its allocations related to climate adaptation as either directly or indirectly addressing climate adaptation. Funding that directly addresses climate adaptation is allocated to the “Climate Change—Adaptation” under SPSD Program Area EG.11 for activities that enhance resilience and reduce the vulnerability to climate change of people, places, and livelihoods. Under this definition, adaptation programs may have the following elements: improving access to science and analysis for decision-making in climate-sensitive areas or sectors; establishing effective governance systems to address climate-related risks; and identifying and disseminating actions that increase resilience to climate change by decreasing exposure or sensitivity or by increasing adaptive capacity. Funding that indirectly addresses climate adaptation is not allocated to a specific SPSD program area. It is funding that is allocated to another SPSD program area and also attributed to the key issue of “Adaptation Indirect,” which is for adaptation activities. The SPSD program area for these activities is not Climate Change—Adaptation, but components of these activities also have climate adaptation effects.
In addition to the SPSD, the State Department and USAID have also identified “key issues” to help describe how foreign assistance funds are used. Key issues are topics of special interest that are not specific to one operating unit or bureau and are not identified, or only partially identified, within the SPSD. As specified in the State Department’s foreign assistance guidance for key issues, “operating units with programs that enhance climate resilience, and/or reduce vulnerability to climate variability and change of people, places, and/or livelihoods are expected to attribute funding to the Adaptation Indirect key issue.”
Operating units use the SPSD and relevant key issues to categorize funding in their operational plans. State guidance requires that any USAID operating unit receiving foreign assistance funding must complete an operational plan each year. The purpose of the operational plan is to provide a comprehensive picture of how the operating unit will use this funding to achieve foreign assistance goals and to establish how the proposed funding plan and programming supports the operating unit, agency, and U.S. government policy priorities. According to the operational plan guidance, State F does an initial screening of these plans.
MDBs play a critical role in bridging the significant funding gap faced by vulnerable developing countries that bear a disproportionate burden of climate adaptation costs—estimated to reach up to 20 percent of GDP for small island nations exposed to tropical cyclones and rising seas. MDBs offer a range of financing options, including direct adaptation investments, green financing instruments, and support for fiscal adjustments to reallocate spending towards climate resilience. To be most sustainably impactful, adaptation support from MDBs should supplement existing aid with conditionality that matches the institutional capacities of recipient countries.
In January 2021, President Biden issued an Executive Order (EO 14008) calling upon federal agencies and others to help domestic and global communities adapt and build resilience to climate change. Shortly thereafter in September 2022, the White House announced the launch of the PREPARE Action Plan, which specifically lays out America’s contribution to the global effort to build resilience to the impacts of the climate crisis in developing countries. Nineteen U.S. departments and agencies are working together to implement the PREPARE Action Plan: State, USAID, Commerce/NOAA, Millennium Challenge Corporation (MCC), U.S. Trade and Development Agency (USTDA), U.S. Department of Agriculture (USDA), Treasury, DFC, Department of Defense (DOD) & U.S. Army Corps of Engineers (USACE), International Trade Administration (ITA), Peace Corps, Environmental Protection Agency (EPA), Department of Energy (DOE), Federal Emergency Management Agency (FEMA), Department of Transportation (DOT), Health and Human Services (HHS), NASA, Export–Import Bank of the United States (EX/IM), and Department of Interior (DOI).
Congress oversees federal climate financial assistance to lower-income countries, especially through the following actions: (1) authorizing and appropriating for federal programs and multilateral fund contributions, (2) guiding federal agencies on authorized programs and appropriations, and (3) overseeing U.S. interests in the programs. Congressional committees of jurisdiction include the House Committees on Foreign Affairs, Financial Services, Appropriations, and the Senate Committees on Foreign Relations and Appropriations, among others.
Transforming On-Demand Medical Oxygen Infrastructure to Improve Access and Mortality Rates
Summary
Despite the World Health Organization’s (WHO) designation of medical oxygen as an essential medicine in 2017, oxygen is still not consistently available in all care settings. Shortages in medical oxygen, which is essential for surgery, pneumonia, trauma, and other hypoxia conditions in vulnerable populations, existed prior to the COVID-19 pandemic and persist today. By one estimate, pre-pandemic, only 20% of patients in low- and middle-income countries (LMICs) who needed medical oxygen received it. The pandemic tremendously increased the need for oxygen, further compounding access issues as oxygen became an indispensable treatment. During the peak of the pandemic, dozens of countries faced severe oxygen shortages due to patient surges impacting an already fragile infrastructure.
The core driver of this challenge is not a lack of funding and international attention but rather a lack of infrastructure to buy oxygen, not just equipment. Despite organizations such as Unitaid, Bill & Melinda Gates Foundation, Clinton Health Access Initiative, UNICEF, WHO and U.S. Agency for International Development (USAID) prioritizing funding and provisions of medical oxygen, many countries still face critical shortages. Even fewer LMICs, such as Brazil, are truly oxygen self-sufficient. A broken and inequitable global oxygen delivery infrastructure inadvertently excludes low-income and rural area representation during the design phase. Furthermore, the current delivery infrastructure is composed of many individual funders and private and public stakeholders who do not work in a coordinated fashion because there is no global governing body to establish global policy, standards, and oversight; identify waste and redundancy; and ensure paths to self-sufficiency. As a result, LMICs are at the mercy of other nations and entities who may withhold oxygen during a crisis or fail to adequately distribute supply. It is time for aid organizations and governments to become more efficient and effective at solving this systemic problem by establishing global governance and investing in and enabling LMICs to become self-sufficient by establishing national infrastructure for oxygen generation, distribution, and delivery.
We propose transforming current interventions by centering the concept known as Oxygen as a Utility (OaaU), which fundamentally reimagines a country’s infrastructure for medical oxygen as a public utility supported by private investment and stable prices to create a functionable, equitable market for a necessary public health good. With the White House Covid Response Team shuttering in the coming months, USAID’s Bureau for Global Health has a unique opportunity to take a global leadership role in spearheading the development of an accessible, affordable oxygen marketplace. USAID should convene a global public-private partnership and governing coalition called the Universal Oxygen Coalition (UOC), pilot the OaaU model in at least two target LMICs (Tanzania and Uttar Pradesh, India), and launch a Medical Oxygen Grand Challenge to enable necessary technological and infrastructure innovation.
Challenge and Opportunity
There is no medical substitute for oxygen, which is used to treat a wide range of acute respiratory distress syndromes, such as pneumonia and pneumothorax in newborns, and noncommunicable diseases, such as asthma, heart failure, and COVID-19. Pneumonia alone is the world’s biggest infectious killer of adults and children, claiming the lives of 2.5 million people, including 740,180 children, in 2019. The COVID-19 pandemic compounded the demand for oxygen, and exposed the lack thereof, with increased death tolls in countries around the world as a result.
For every COVID-19 patient who needs oxygen, there are at least five other patients who also need it, including the 7.2 million children with pneumonia who enter LMIC hospitals each year. [Ehsanur et al, 2021]. Where it is available, there are often improperly balanced oxygen distribution networks, such as high-density areas being overstocked while rural areas or tertiary care settings go underserved. Only 10% of hospitals in LMICs have access to pulse oximetry and oxygen therapy, and those better-resourced hospitals tend to be in larger cities closer to existing oxygen delivery providers.
This widespread lack of access to medical oxygen in LMICs threatens health outcomes and well-being, particularly for rural and low-income populations. The primary obstacle to equitable oxygen access is lack of the necessary digital infrastructure in-country. Digital infrastructure provides insights that enable health system managers and policymakers to effectively establish policy, manage the supply of oxygen to meet needs, and coordinate work across a complex supply chain composed of various independent providers. Until replicable and affordable digital infrastructure is established, LMICs will not have the necessary resources to manage a national oxygen delivery system, forecast demand, plan for adequate oxygen production and procurement, safeguard fair distribution, and ensure sustainable consumption.
Oxygen can be delivered in a number of forms—via concentrators, cylinders, plants, or liquid—and the global marketplace encompasses many manufacturers and distributors selling in multiple nations. Most oxygen providers are for-profit organizations, which are not commercially incentivized to collaborate to achieve equal oxygen access, despite good intentions. Many of these same manufacturers also sell medical devices to regulate or deliver oxygen to patients, yet maintaining the equipment across a distributed network remains a challenge. These devices are complex and costly, and there are often few trained experts in-country to repair broken devices. Instead of recycling or repairing devices, healthcare providers are often forced to discard broken equipment and purchase new ones, contributing to greater landfill waste and compounding health concerns for those who live nearby.
Common contributing causes for fragmented oxygen delivery systems in LMICs include:
- No national digital infrastructure to connect, track, and monitor medical oxygen supply and utilization, like an electrical utility to forecast demand and ensure reliable service delivery.
- No centralized way to monitor manufacturers, distributors, and the various delivery providers to ensure coordination and compliance with local policy.
- In many cases, no established local policy for oxygen and healthcare regulation or no means to enforce local policy.
- Lack of purchasing options for healthcare providers, who are often forced to buy whichever oxygen devices are available versus the type of source oxygen that best fits their needs (i.e., concentrator or liquid) due to cumbersome tender systems and lack of coordination across markets.
- Lack of trained experts to maintain and repair devices, including limited national standardized certification programs, resulting in the premature disposal of costly medical devices contributing to waste issues. Further, lack of maintenance fuels the vicious cycle of LMICs requiring more regular funding to buy oxygen devices, which can increase reliance on third parties to sustain oxygen needs rather than domestic demand and marketplaces.
Medical oxygen investment is a unique opportunity to achieve global health outcomes and localization policy objectives. USAID invested $50 million to expand medical oxygen access through its global COVID-19 response for LMIC partners, but this investment only scratches the surface of what is needed to deliver self-sustainment. In response to oxygen shortages during the peaks of the pandemic, the WHO, UNICEF, the World Bank, and other donors shipped hundreds of thousands of oxygen concentrators to help LMICs deal with the rise in oxygen needs. This influx of resources addressed the interim need but did not solve the persisting healthcare system and underlying oxygen infrastructure problems. In 2021, the World Bank made emergency loans available to LMICs to help them shore up production and infrastructure capabilities, but not enough countries applied for these loans, as the barriers to solve these infrastructure issues are complex, difficult to identify without proper data and digital infrastructure to identify supply chain gaps, and hard to solve with a single cash loan.
Despite heavy attention to the issue of oxygen access in LMICs, current spending does not go far enough to set up sustainable oxygen systems in LMICs. Major access and equity gaps still persist. In short, providing funding alone without a cohesive, integrated industrial strategy cannot solve the root problem of medical oxygen inequality.
USAID recently announced an expanded commitment in Africa and Asia to expand medical oxygen access, including market-shaping activities and partnerships. Since the pandemic began, USAID has directed $112 million in funding for medical oxygen to 50 countries and is the largest donor to The Global Fund, which has provided the largest international sums of money (more than $600 million) to increase medical oxygen access in over 80 countries. In response to the pandemic’s impacts on LMICs, the ACT-Accelerator (ACT-A) Oxygen Emergency Taskforce, co-chaired by Unitaid and the Wellcome Trust, has provided $700 million worth of oxygen supplies to over 75 countries and catalyzed large oxygen suppliers and NGO leaders to support LMICs and national healthcare ministries. This task force has brought together industry, philanthropy, NGO, and academic leaders. While USAID is not a direct partner, The Global Fund is a primary donor to the task force.
Without a sea change in policy, however, LMICs will continue to lack the support required to fully diagnosis national oxygen supply delivery system bottlenecks and barriers, establish national regulation policies, deploy digital infrastructures, change procurement approaches, enable necessary governance changes, and train in-country experts to ensure a sustained, equitable oxygen supply chain. To help LMICs become self-sufficient, we need to shift away from offering a piecemeal approach (donating money and oxygen supplies) to a holistic approach that includes access to a group of experts , funding for oxygen digital infrastructure systems, aid to develop national policy and governance mechanisms, and support for establishing specialty training and certification programs so that LMICs can self-manage their own medical oxygen supply chain. Such a development policy initiative relies on the Oxygen as a Utility framework, which focuses on creating a functional, equitable market for medical oxygen as a necessary public good. When achieved successfully, OaaU facilitates one fair rate for end-to-end distribution within a country, like other public utilities such as water and electricity.
A fully realized OaaU model within a national economy would integrate and streamline most aspects of oxygen delivery, from production to distribution of both the oxygen and the devices that dispense it, to training of staff on when to administer oxygen, how to use equipment, and equipment maintenance. This proposed new model coordinates industry partners, funders, and country leaders to focus on end-to-end medical oxygen delivery as an affordable, accessible utility rather than an in-kind development good. OaaU centers predictability, affordability, and efficiency for each stakeholder involved in creating sustainable LMIC medical oxygen supply chains. At its core, OaaU is about increasing both access and reliability by providing all types of oxygen at negotiated, market-wide, affordable, and predictable prices through industry partners and local players. This new business model would be sustainable by charging subscription and pay-per-use fees to serve the investment by private sector providers, each negotiated by Ministries of Health to empower them to manage their own country’s oxygen needs. This new model will incorporate each stakeholder in an LMIC’s healthcare system and facilitate an open, market-based negotiation to achieve affordable, self-sufficient medical oxygen supply chains.
Initial investment is needed to create a permanent oxygen infrastructure in each LMIC to digitally transform the tender system from an equipment and service or in-kind aid model to buying oxygen as a utility model. An industry business model transformation of this scale will require multistakeholder effort to include in-country coordination. The current oxygen delivery infrastructure is composed of many individual funders and private and public stakeholders who do not work in a coordinated fashion. At this critical juncture for medical oxygen provision, USAID’s convening power, donor support, and expertise should be leveraged to better direct this spending to create innovative opportunities. The Universal Oxygen Coalition would establish global policy, standards, and oversight; identify waste and redundancy; and ensure viable paths to oxygen self-sufficiency in LMICs. The UOC will act similarly to electric cooperatives, which aggregate supplies to meet electricity demand, ensuring every patient has access to oxygen, on demand, at the point of care, no matter where in the world they live.
Plan of Action
To steward and catalyze OaaU, USAID should leverage its global platform to convene funders, suppliers, manufacturers, distributors, health systems, financial partners, philanthropy, and NGOs and launch a call to action to mobilize resources and bring attention to medical oxygen inequality. USAID’s Bureau for Global Health, along with the its Private Sector Engagement Points of Contact, and the State Department’s Office of Global Partnerships should spearhead the UOC coalition. Using USAID’s Private Sector Engagement Strategy and EDGE fund as a model, USAID can serve as a connector, catalyzer, and lead implementer in reforming the global medical oxygen marketplace. The Bureau for Global Health should organize the initial summit, calls to action, and burgeoning UOC coalition because of its expertise and connections in the field. We anticipate that the UOC would require staff time and resources, which could be funded by a combination of private and philanthropic funding from UOC members in addition to some USAID resources.
To achieve the UOC vision, multiple sources of funding could be leveraged in addition to Congressional appropriation. In 2022, State Department and USAID funding for global health programs, through the Global Health Programs (GHP) account, which represents the bulk of global health assistance, totaled $9.8 billion, an increase of $634 million above the FY21 enacted level. In combination with USAID’s leading investments in The Global Fund, USAID could deploy existing authorities and funding from Development Innovation Ventures’ (DIV) and leverage Grand Challenge models like Saving Lives at Birth to create innovation incentive awards already authorized by Congress, or the newly announced EDGE Fund focused on flexible public-private sector partnerships to direct resources toward achieving equitable oxygen access for all. These transformative investments would also serve established USAID policy priorities like localization. UOC would work with USAID and the Every Breath Counts Initiative to reimagine this persistent problem by bringing essential players—health systems, oxygen suppliers, manufacturers and/or distributors, and financial partners—into a unified holistic approach to ensure reliable oxygen provision and sustainable infrastructure support.
Recommendation 1. USAID’s Bureau for Global Health should convene the Universal Oxygen Coalition Summit to issue an OaaU co-financing call to action and establish a global governing body.
The Bureau for Global Health should organize the summit, convene the UOC coalition, and issue calls to action to fund country pilots of OaaU. The UOC coalition should bring together LMIC governments; local, regional, and global private-sector medical oxygen providers; local service and maintenance companies; equipment manufacturers and distributors; health systems; private and development finance; philanthropy organizations; the global health NGO community; Ministries of Health; and in-country faith-based organizations.
Once fully established, the UOC would invite industry coalition members to join to ensure equal and fair representation across the medical oxygen delivery care continuum. Potential industry members include Air Liquide, Linde, Philips, CHART, Praxair, Gulf Cryo, Air Products, International Futures, AFROX, SAROS, and GCE. Public and multilateral institutions should include the World Bank, World Health Organization, UNICEF, USAID country missions and leaders from the Bureau for Global Health, and selected country Ministries of Health. Funders such as Rockefeller Foundation, Unitaid, Bill & Melinda Gates Foundation, Clinton Health Access Initiative, and Wellcome Trust, as well as leading social enterprises and experts in the oxygen field such as Hewatele and PATH, should also be included.
UOC members would engage and interact with USAID through its Private Sector Engagement Points of Contact, which are within each regional and technical bureau. USAID should designate at least two points of contact from a regional and technical bureau, respectively, to lead engagement with UOC members and country-level partners. While dedicated funds to support the UOC and its management would be required in the long term either from Congress or private finance, USAID may be able to deploy staff from existing budgets to support the initial stand-up process of the coalition.
Progress and commitments already exist to launch the UOC, with Rockefeller Philanthropy Advisors planning to bring fiscal sponsorship as well as strategy and planning for the formation of the global coalition to the UOC with PATH providing additional strategic and technical functions for partners. The purpose of the UOC through its fiscal sponsor is to act as the global governing body by establishing global policy, standards, oversight controls, funding coordination, identifying waste & redundancy, setting priorities, acting as advisor and intermediary when needed to ensure LMIC paths to self-sufficiency are available. UOC would oversee and manage country selection, raising funding, and coordination with local Ministries of Health, funders, and private sector providers.
Other responsibilities of the UOC may include:
- Issue feasibility studies to assess technology gaps in target countries. This research would inform future challenges, contracts, prioritization, design, and focus.
- Advise LMICs on identifying barriers and knowing best next steps.
- Establish an official framework of best practices for OaaU that includes core metrics of success and replicable models.
The first UOC Summit will issue a call to action to make new, significant commitments from development banks, philanthropies, and aid agencies to co-finance OaaU pilot programs, build buy-in within target LMICs, and engage in market-shaping activities and infrastructure investments in the medical oxygen supply chain. The Summit could occur on the sidelines of the Global COVID-19 Summit or the United Nations General Assembly. Summit activities and outcomes should include:
- Announce the launch and secure financial commitments from public and private funds for piloting OaaU in at least one national context.
- Identify and prioritize criteria for selecting pilot locations (regions or nations) for OaaU and select the initial country(s) for holistic oxygen self-sufficiency investment.
- Create the UOC Board representing manufacturers, global health experts, LMIC leaders, funders, multilateral institutions, and health providers who are empowered to identify geographic areas most in need of oxygen investment, issue market-specific grants and open innovation competitions, and leverage pooled public and private funds.
- Research, prioritize, and select at least two models of OaaU within a national marketplace to focus attention of all stakeholders on fixing the oxygen marketplace.
Recommendation 2. The UOC should establish country prioritization based on need and readiness and direct raised funds toward pilot programs.
USAID should co-finance an OaaU pilot model through investments in domestic supply chain streamlining and leverage matched funds from development bank, private, and philanthropic dollars. This fund should be used to invest in the development of a holistic oxygen ecosystem starting in Tanzania and in Uttar Pradesh, India, so that these regions are prepared to deliver reliable oxygen supply, catalyzing broad demand, business activity, and economic development.
The objective is to deliver a replicable global reference model for streamlining the supply chain and logistics, eventually leading to equitable oxygen catering to the healthcare needs that can be rolled out in other LMICs and improve lives for the deprived. The above sites are prioritized based on their readiness and need as determined by the 2020 PATH Market Research Study supported by the Bill and Melinda Gates Foundation. We estimate that $495 million for the pilots in both nations would provide oxygen for 270 million people, which equates to less than $2 per person. The UOC should:
- Invest in local providers: This will generate economic development and high-paying jobs in-country and throughout the supply chain.
- Spur localized innovation and digital transformation: Foster locally driven innovation by in-country and regional systems integrators, especially in digital transformation of oxygen generation, distribution, and delivery. Solutions should include new digital tools for aggregation of supply and demand and real-time command and control to radically improve access to medical oxygen on demand.
- Create an in-country deployment coalition for each pilot country: Because oxygen marketplaces are unique to each context, having a market-based deployment coalition in each country that involves private, public, and social sector partners is critical to coordinating the deployment of resources and maintaining implementation efforts. The deployment coalition could be operated out of or supervised by a USAID Country Mission.
- Provide pilot model funding to enable Ministries of Health and the deployment coalition to streamline and fix supply chains.
- Issue calls to action for interested parties and stakeholders to submit plans to address both the immediate medical oxygen needs in the country of choice and the long-term infrastructure barriers. These plans could help inform strategy for deploying resources and making oxygen infrastructure investments.
This effort will result in a sustainable oxygen grid in LMICs to produce revenue via subscription and pay-per-use model, reducing the need for aid organization or donor procurement investment on an annual basis. To create the conditions for OaaU, the UOC will need to make a one-time investment to create infrastructure that can provide the volume of oxygen a country needs to become oxygen self-sufficient. This investment should be backed by the World Bank via volume usage guarantees similar to volume usage guarantees for electricity per country. The result will shift the paradigm from buying equipment to buying oxygen.
Recommendation 3. The UOC and partner agencies should launch the Oxygen Access Grand Challenge to invest in innovations to reduce costs, improve maintenance, and enhance supply chain competition in target countries.
We envision the creation of a replicable solution for a self-sustaining infrastructure that can then serve as a global reference model for how best to streamline the oxygen supply chain through improved infrastructure, digital transformation, and logistics coordination. Open innovation would be well-suited to priming this potential market for digital and infrastructure tools that do not yet exist. UOC should aim to catalyze a more inclusive, dynamic, and sustainable oxygen ecosystem of public- and private-sector stakeholders.
The Grand Challenge platform could leverage philanthropic and private sector resources and investment. However, we also recommend that USAID deploy some capital ($20 million over four years) for the prize purse focused on outcomes-based technologies that could be deployed in LMICs and new ideas from a diverse global pool of applicants. We recommend the Challenge focus on the creation of digital public goods that will be the digital “command and control” backbone of a OaaU in-country. This would allow a country’s government and healthcare system to know their own status of oxygen supply per a country grid and which clinic used how much oxygen in real time and bill accordingly. Such tools do not yet exist at affordable, accessible levels in LMICs. However, USAID and its UOC partners should scope and validate the challenge’s core criteria and problems, as they may differ depending on the target countries selected.
Activities to support the Challenge should include:
- Assessing technology and cost gaps in target partner countries in healthcare infrastructure, with a particular focus on supply chains and oxygen provision. This research would inform the Challenge design and focus.
- Creating partnerships with LMICs to implement promising innovations in pilots and secure advanced market commitments from healthcare ministries, the private sector, and multilateral or private financing to ensure viable pathways to scale for solutions.
- Establishing an official framework of best practices for OaaU that includes core metrics of success and replicable models that interested healthcare ministries could use to develop a system in their own nations.
Conclusion
USAID can play a catalytic role in spearheading the creation and sustainment of medical oxygen through a public utility model. Investing in new digital tools for aggregation of supply and demand and real-time command and control to radically improve access to medical oxygen on demand in LMICs can unlock better health outcomes and improve health system performance. By piloting the OaaU model, USAID can prove the sustainability and scalability of a solution that can be a global reference model for streamlining medical oxygen supply chain and logistics. USAID and its partners can begin to create sustained change and truly equitable oxygen access. Through enhancing existing public-private partnerships, USAID can also cement a resilient medical oxygen system better prepared for the next pandemic and better equipped to deliver improved health outcomes.
References
- Pneumonia in Children Statistics – UNICEF DATA
- Ann Danaiya Usher (2021). Medical oxygen crisis: a belated COVID-19 response. The
Lancet, World Report. - Lam F., Stegmuller A.,Chouz V.B., Grahma H.R. (2021). Oxygen systems strengthening as
an intervention to prevent childhood deaths due to pneumonia in low-resource settings:
systematic review, meta-analysis and cost-effectiveness. BMJ Global Health Journals - AD Usher: Medical Oxygen crisis: a belated COVID-19 response (2021) The Lancet Global
Health. - Nair H, Simoes EA, Rudan I, Gessner BD, Azziz-Baumgartner E, Zhang JS et al.
(2013) Global and regional burden of hospital admissions for severe acute lower respiratory
infections in young children in 2010: a systematic analysis. Lancet 381: 1380–90.
10.1016/S0140-6736(12)61901-1 - Liu L, Johnson HL, Cousens S, Perin J, Scott S, Lawn JE et al. (2012) Global, regional, and national causes of child mortality: An updated systematic analysis for 2010 with time trends since 2000. Lancet 379: 2151–61. 10.1016/S0140-6736(12)60560-1
- UNEP report. Africa waste management outlook. (2018)
- T Duke, SM Gramham, NN Cherian, AS Ginsburg, M English, S Howie, D Peel, PM Enarson,
IH Wilson, and W Were, the Union Oxygen Systems Working Group (2010) Oxygen is an
essential medicine: A call for international action. - Unitaid press release. COVID-19 emergency impacting more than half a million people in low-
and middle-income countries every day, as demand surges (2021)
The OaaU approach integrates and streamlines most aspects of oxygen delivery, just as integrated power grids grew into public utilities through government investment and public-private partnerships built on technological development to manage them. With an OaaU approach, investments would be made in oxygen digital grid design, build, interoperable connectivity across markets, staff training, demand forecasting and development of a longitudinal sustainable plan. Through this model, an increased number of oxygen suppliers would compete through auctions designed to drive down cost. Governments would receive a lower fixed price in exchange for offering a firm commitment to purchase a pre-established amount of oxygen, services, and equipment to provide oxygen over a long-time horizon. Financial partners guarantee the value of these commitments to reduce the risk that countries will default on their payments, seeking to encourage the increased competition that turns the wheels of this new mechanism. Providing a higher-quality, lower-cost means of obtaining medical oxygen would be a relief for LMICs. Additionally, we would anticipate the government to play a greater role in regulation and oversight which would provide price stability, affordability, and adequate supply for markets—just like how electricity is regulated.
First, oxygen is a complex product that can be generated by concentrators, cylinders, plants, and in liquid oxygen form. For a country to become oxygen self-sufficient, it needs all types of oxygen, and each country has its own unique combination of needs based on healthcare systems, population needs, and existing physical infrastructure. If a country has an excellent transportation system, then delivery of oxygen is the better choice. But if a country has a more rural population and no major highways, then delivery is not a feasible solution.
The oxygen market is competitive and consists of many manufacturers, each of which bring added variations to the way oxygen is delivered. While WHO-UNICEF published minimal technical specifications and guidance for oxygen therapy devices in 2019, there remains variation in how these devices are delivered and the type of data produced in the process. Additionally, oxygen delivery requires an entire system to ensure it safely reaches patients. In most cases, these systems are decentralized and independently run, which further contributes to service and performance variation. Due to layers of complexity, access to oxygen includes multiple challenges in availability, quality, affordability, management, supply, human resources capacity, and safety. National oversight through a digital oxygen utility infrastructure that requires the coordination and participation of the various oxygen delivery stakeholders would address oxygen access issues and enable country self-sustainment.
Given that oxygen provides areturn of US $50 per disability-adjusted life year, medical oxygen investment is a meaningful opportunity for development banks, foreign assistance agencies, and impact investors. The OaaU business model transformation will be a major step toward oxygen availability in the form of oxygen on-demand in LMICs. Reliable, affordable medical oxygen can strengthen the healthcare infrastructure and improve health outcomes. Recent estimates indicate every year about 120–156 million cases of acute lower respiratory infections occur globally in children under five, with approximately 1.4 million resulting in death. More than 95% of these deaths occur in low- and middle-income countries (Nair, 2013; Lui, 2012).
Unlike prior approaches, OaaU is a business model transformation from partial solutions to integrated solutions with all types of oxygen, just like the electricity sector transformed into an integrated grid of all types of electricity supply. From there, the medical facilities will buy oxygen, not equipment—just like you buy amounts of electricity, not a nuclear power plant.
Saving 3.1 Million Lives a Year with a President’s Emergency Plan to Combat Acute Childhood Malnutrition
Summary
Like HIV/AIDS, acute childhood malnutrition is deadly but easily treatable when the right approach is taken. Building on the success of PEPFAR, the Biden-Harris Administration should launch a global cross-agency effort to better fund, coordinate, research, and implement malnutrition prevention and treatment programs to save millions of children’s lives annually and eventually eliminate severe acute malnutrition.
Children with untreated severe acute malnutrition are 9 to 11 times more likely to die than their peers and suffer from permanent setbacks to their neurodevelopment, immune system, and future earnings potential if they survive. Effective programs can treat children for around $60 per child with greater than 90 percent recovery rates. However, globally, only about 25–30 percent of children with moderate and severe acute malnutrition have access to treatment. Every year, 3.1 million children die due to malnutrition-related causes, and 45% of all deaths of children under five are related to malnutrition, making it the leading cause of under-five deaths.
In 2003, a similar predicament existed: the HIV/AIDS epidemic was causing millions of deaths in sub-Saharan Africa and around the world, despite the existence of highly effective treatment and prevention methods. In response, the Bush Administration created the President’s Emergency Plan for AIDS Relief (PEPFAR). PEPFAR has proven a major global health success, saving an estimated 30 million lives since 2003 through over $100 billion in funding.
The Biden-Harris Administration should establish a President’s Emergency Plan for Acute Childhood Malnutrition (PEPFAM) in the Office of Global Food Security at the State Department to clearly elevate the problem of acute childhood malnutrition, leverage new and existing food security and health programs to serve U.S. national security and humanitarian interests, and save the lives of up to 3.1 million children around the world, every year. PEPFAM could serve as a catalytic initiative to harmonize the fight against malnutrition and direct currently fragmented resources toward greater impact.
Challenge and Opportunity
United Nations Sustainable Development Goal (SDG) 2.2 outlines goals for reducing acute malnutrition, ambitiously targeting global rates of 5 percent by 2025 and 3 percent (a “virtual elimination”) by 2030. Due to climate change, the COVID-19 pandemic, and conflicts like the war in Ukraine, global rates of malnutrition remain at 8 percent and are forecast to become worse, not better. Globally, 45.4 million children suffer from acute malnutrition, 13.6 million of whom are severely acutely malnourished (SAM). If current trends persist until 2030, an estimated 109 million children will suffer from permanent cognitive or physiological stunting, despite the existence of highly effective and relatively cheap treatment.
Providing life-saving treatment around the world serves a core American value of humanitarianism and helps meet commitments to the SDGs. The United States Agency for International Development (USAID) recently announced a commitment to purchase ready-to-use therapeutic food (RUTF), a life-saving food, on the sidelines of the UN General Assembly, demonstrating a prioritization of global food security. Food security is also a priority for the Biden Administration’s approach to national security. The newly released National Security Strategy dedicates an entire section to food insecurity, highlighting the urgency of the problem and calling on the United States and its global partners to work to address acute needs and tackle the extraordinary humanitarian burden posed by malnutrition. The Office of Global Food Security at the U.S. Department of State also prioritizes food security as an issue of national security, leading and coordinating diplomatic engagement in bilateral, multilateral, and regional contexts. At a time when the United States is competing for its vision of a free, open, and prosperous world, addressing childhood malnutrition could serve as a catalyst to achieve the vision articulated in the National Security Strategy and at the State Department.
“People all over the world are struggling to cope with the effects of shared challenges that cross borders—whether it is climate change, food insecurity, communicable diseases, terrorism, energy shortages, or inflation. These shared challenges are not marginal issues that are secondary to geopolitics. They are at the very core of national and international security and must be treated as such.”
U.S. 2022 National Security Strategy
Tested, scalable, and low-cost solutions exist to treat children with acute malnutrition, yet the platform and urgency to deliver interventions at scale does not. Solutions such as community management of acute malnutrition (CMAM), the gold standard approach to malnutrition treatment, and other intentional strategies like biofortification could dramatically lower the burden of global childhood malnutrition. Despite the 3.1 million preventable deaths that occur annually related to childhood malnutrition and the clear threat that food insecurity poses to U.S. national security, we lack an urgent platform to bring these low-cost solutions to bear.
While U.S. government assistance to combat food insecurity and malnutrition is a priority, funding and coordination are not centralized. The U.S. has committed over $10 billion to address global food insecurity, allocating dollars to USAID, Feed the Future, the U.S. Department of Agriculture (USDA), and others. Through the recently signed Global Malnutrition Prevention and Treatment Act of 2021, Congress took a step forward by authorizing USAID to have greater authority in targeting nutrition aid to areas of greatest need and greater flexibility to coordinate activities across the agency and its partners. In accordance with the agency’s Global Nutrition Coordination Plan, Congress also established the Nutrition Leadership Council, chaired by the Bureau for Resilience and Food Security to coordinate and integrate activities solely within USAID. Multilateral and private sector partners also dedicate resources to food security: the Gates Foundation committed $922 million toward global nutrition and food systems, and UNICEF created a Nutrition Match Fund to incentivize funding to combat severe acute malnutrition. These lines of effort are each individually important, but could be more impactful if aligned. A President’s Emergency Plan for malnutrition could harmonize these separate funding streams and authorities and mobilize multilateral and private sector partners to prevent and treat malnutrition and food insecurity.
Drawing on the strengths of the PEPFAR model to combat HIV/AIDS at scale while driving down costs for treatment, PEPFAM could revolutionize how resources are spent while scaling sustainable and cost-effective solutions to childhood malnutrition, saving millions of lives every year. Under this model, significantly more—and, optimally, all—children suffering from acute malnutrition would have access to treatment. This would make dramatic progress toward global food security and U.S. national security priorities.
Plan of Action
President Biden should declare a global childhood malnutrition emergency and announce the creation of the President’s Emergency Plan for Acute Childhood Malnutrition. Using PEPFAR as a model, PEPFAM could catalyze cost-effective solutions to save millions of lives every year. When President Bush mobilized support for PEPFAR in his 2003 State of the Union, he declared, “We must remember our calling, as a blessed country, is to make the world better,” and called for interagency support for an “Emergency Plan” for HIV/AIDS relief and Congressional support to commit $15 billion over the next five years to launch PEPFAR.
President Biden should follow a similar path and announce PEPFAM in a similarly high-profile speech—the 2023 State of the Union address, for example—to elevate the problem of acute childhood malnutrition to the American people and the U.S. government and offer a clear call to action through an executive order directing an interagency task force to develop a 24-month strategic plan within 180 days. The initial stages of PEPFAM and corresponding executive branch activities can be guided by the following recommendations.
Recommendation 1. Name a White House PEPFAM czar and task the Office of Global Food Security at the State Department to coordinate cross-agency support, intended personnel, agencies, and roles involved.
A Senior Advisor on the White House’s National Security Team at the Office of Science and Technology Policy would serve as the White House czar for PEPFAM and would (1) steer and lead the initiative, (2) organize an interagency task force, and (3) coordinate PEPFAM’s strategic focus by engaging multiple federal agencies, including:
- USAID’s Bureau of Resilience and Food Security
- State Department’s Office of Global Food Security
- State Department’s Office of the Global AIDS Coordinator and Health Diplomacy (OGAC)
- Department of Health and Human Service’s Office of Global Affairs
- Department of Agriculture’s Foreign Agricultural Service
- The White House National Security Council (and/or other relevant offices)
The Office of the Global AIDS Coordinator and Health Diplomacy at the State Department (OGAC) manages the high-level execution of PEPFAR by dictating strategic direction and coordinating agencies. The PEPFAM executive order will set up a similar infrastructure at the Office of Global Food Security at the State Department to:
- Coordinate activities and funding across the U.S. government, the private sector, and multilateral organizations
- Approve all activities related to PEPFAM
- Oversee accountability and monitoring and evaluation
- Provide strategic direction for the program
USAID is also well positioned to play a leading role given its current support of global food and nutrition programming. Several of USAID’s portfolios are central to PEPFAM’s aims, including Agriculture and Food Security, Nutrition, Global Health, Water and Sanitation, and Humanitarian Assistance. The offices that support these portfolios should provide technical expertise in the realm of food and nutrition, existing connections to good program implementers in various country contexts, monitoring and evaluation capacity to track implementer’s progress toward goals, and strategic direction.
The Office of Global Food Security and the PEPFAM czar should delegate authority for the program across government agencies, private partners (e.g., Gates Foundation), and multilateral organizations (e.g., World Food Programme). The Office would coordinate interagency action to support PEPFAM’s implementation and evaluation as well as identify agencies that are best placed to lead each component of the effort.
Recommendation 2. Present initial, strategic action plan to build and sustain PEPFAM.
The PEPFAM interagency task force, described above, should develop a strategic plan targeting an initial set of actions to align with existing global food security and childhood malnutrition priorities and identify opportunities to redirect existing resources toward scalable, high-impact solutions like CMAM. USAID already invests millions of dollars each year in initiatives like Feed the Future that support global food security while overseeing cross-agency implementation and harmonization of the Global Food Security Strategy. These efforts and funding should be rolled under the umbrella of PEPFAM to better align treatment and prevention interventions, strategically coordinate resources across the government, and improve a focus on impact.
Recommendation 3. Announce discrete, evidence-driven goals for PEPFAM.
These goals include:
- Catalyze global funding and direct resources toward effective, low-cost solutions to address acute childhood malnutrition.
- Provide sustained access to treatment for children suffering from acute malnutrition, both moderate and severe, even in geographic areas that are not designated as crises or emergency situations.
- Scale proven, cost-effective prevention interventions to reduce the burden of childhood malnutrition and invest in research and evaluation to identify new prevention mechanisms.
- Coordinate and conduct targeted humanitarian efforts to triage and respond rapidly to emergent situations of famine/starvation.
- Invest in research, innovation, and monitoring and evaluation to ensure that U.S. government and global funds are put toward the most cost-effective (e.g., cheap and effective) interventions to maximize the impact of existing and additional funds.
Recommendation 4. Establish a coordination framework between PEPFAM, multilateral agencies, and private sector partners to mobilize and harmonize resources.
The Office of Global Food Security and USAID should build on current momentum to bring multilateral and private partners behind PEPFAM. USAID has recently announced a series of partnerships with large philanthropic organizations like the Gates Foundation, Aliko Dangote Foundation, and Eleanor Crook Foundation (to name a few), as well as other countries and multilateral organizations at UNGA. Much like with PEPFAR, PEPFAM could rely on the support of external partners as well as federal funds to maximize the impact of the program.
Recommendation 5. Create an international council to set technical standards so that money goes to the most effective programs possible.
The Office of Global Food Security, USAID, and PEPFAM should spearhead the development of an international technical council (that could be housed under the UN, the World Health Organization, or independently) to set standards for malnutrition prevention and treatment programming. Malnutrition treatment is already cost-effective, but it could be made even cheaper and more effective through innovation. Even when promising new interventions are identified, the process of disseminating and scaling of existing, proven best practices innovations doesn’t function optimally.
Treatment guidelines issued by the WHO and national governments are slow to be updated, meaning that highly effective interventions can take years to be adopted and, even then, are adopted in a piecemeal fashion. Other implementers may be too wedded to their operational practices to consider making a change unless standards are updated or innovations from other implementers are actively socialized.
An international technical council would disseminate and scale best practices discovered in the processes of implementation and research. If funders like the U.S. government commit to only funding organizations that promptly adopt these standards, they can maximize the impact of existing funding by ensuring that every dollar goes toward the most cost-effective ways of saving lives. This body could ideally speed the sharing and implementation of practices that could allow more children to be treated effectively, at lower costs.
Recommendation 6. Direct existing child malnutrition assistance through PEPFAM to ensure coordinated impact and seek permanent funding from Congress for PEPFAM.
The executive order will create the momentum to establish PEPFAM, but legislative authorization is required to make it sustainable. The strategic plan should lay out efforts to build Congressional support for funding legislation.
Congress will play a key role in PEPFAM implementation by appropriating funds. Under PEPFAR, Congress appropriates money directly to OGAC at the Department of State, which disburses it to other agencies. In 2003, Congress supported President Bush’s request for $15 billion in PEPFAR funding by passing the Leadership Act that authorized yearly contributions to the Global Fund from 2004 to 2008. Congress has subsequently reauthorized the program through FY2023. Each year, the OGAC presents a request of funding needed for recipient countries and programs to the President, who then forwards the request to Congress for reauthorization. The PEPFAM process should mirror this structure.
At the UNGA in 2022, President Biden announced over $2.9 billion in new assistance to address global food insecurity, building on the $6.9 billion in U.S. government assistance already committed in 2021. Last year, President Biden also announced a $10 billion, multiyear investment to promote food systems transformation, including a $5 billion commitment to Feed the Future specifically. Instead of fractured funding to different initiatives, these funds should be harmonized under PEPFAM, with dollars allocated to the PEPFAM task force to create a centralized two-year strategy to combat malnutrition.
Conclusion
This program would have a series of positive effects. First, and most obviously, PEPFAM would save up to 3.1 million lives every year and bring together resources and goals around food security that are currently fractured across the federal government, increasing the effectiveness of U.S. aid dollars globally. Second, PEPFAM, like PEPFAR, would make existing interventions more effective by unlocking cost savings and innovation at scale. Third, at a time when the United States is competing for its vision of a free, open, and prosperous world, PEPFAM could play a key role in achieving the mission of the National Security Strategy.
Over time, more comprehensive treatment coverage and prevention efforts could also lead to the elimination of severe acute malnutrition by preventing cases and catching those that approach moderate acute malnutrition or have already fallen into it. PEPFAM would save an estimated 27.9 million lives over the same time scale as PEPFAR. Millions of children die every year while a cheap and effective solution exists. PEPFAM could change that.
From 2003 to present day, PEPFAR has spent billions of dollars and saved millions of lives. This table compares the estimated costs and outcomes of PEPFAR with PEPFAM. Because malnutrition treatment is cheaper than HIV/AIDS treatment and there is a higher caseload, there is a high-leverage opportunity to save lives.
| PEPFAR (HIV/AIDS) | PEPFAM (Childhood Malnutrition) | |
| Average Cost of Treatment per Person | $367,134 | $60 |
| Number of Cases | 38.4 million | 45.4 million |
| Program Cost (estimated yearly) | $5.7 billion (USD) | $4 billion (USD) |
| Lives Saved (estimated yearly) | 1.6 million | 1.5 million |
Costs for PEPFAM are difficult to project precisely, because the program is likely to become more cost-effective over time as efforts to prevent cases start to work and research and development result in cheaper and more effective treatment. The projections above operate under the most pessimistic assumptions that no improvements to cost or effectiveness are made over time. This graph illustrates a similar the expansion of PEPFAR services, even under flat budgets thanks to this same self-improvement over time.

PEPFAM is similar: more comprehensive treatment coverage and prevention efforts could lead to the elimination of severe acute malnutrition by preventing cases and catching those that approach moderate acute malnutrition or have already fallen into it. That means that the program should become cheaper over time, as more cases are identified earlier when they are cheaper to treat, and more cases are prevented, both by prevention programs and general economic development. Research and innovation can similarly cut down on the costs and improve the effectiveness of malnutrition treatment and prevention over time.
The lack of attention to childhood malnutrition in non-emergency/non-crisis zones results in millions of preventable deaths each year. Declaring an emergency would put pressure on other organizations, media outlets, and NGOs to devote more resources to food security. The international community is keen to respond to food crises in emergency contexts, especially among children. USAID and the UN recently committed millions of dollars for the procurement of ready-to-use therapeutic food (RUTF) to combat emergency risks like the war in Ukraine and conflicts in places like Ethiopia. But the unfortunate truth is that even outside of newsworthy emergencies, acute malnutrition remains a daily emergency in many places around the world. Malnutrition rates are just as high in states and countries that neighbor emergency zones as in the crisis-hit places themselves, partially as a result of movement of internally displaced people. While funding acute malnutrition in relatively mundane circumstances (e.g., poverty-stricken states in Nigeria) may make less headlines than emergency food aid, it’s equally needed.
Currently, only 1 percent of U.S. global health spending is put toward nutrition. Only 25–30 percent of children globally have access to treatment as a result of underfunded programs and a subsequent lack of resources and geographic coverage.
Treatment is only effective if implemented well. Right now, funding goes to a range of programs that fail to meet Sphere Standards of 75 percent recovery rates. Large-scale funders like UNICEF have internal commitments to spend a certain amount of their budgets on ready-to-use therapeutic food (RUTF) a year, which means that their hands are tied when working in contexts with poor implementing partners (e.g., corrupt governments). At the same time, NGOs like Alliance for International Medical Action and Médecins Sans Frontières achieve recovery rates of more than 95 percent. More investment in quality implementation capacity is needed; otherwise, scarce existing resources will continue to be wasted.
There’s a growing movement to implement interventions that catch children on the border of malnutrition or improve conditions that lead to malnutrition in the first place (e.g., infant and young child feeding circles, exclusive breastfeeding counseling). These programs are exciting, but the evidence base for impact at this point is minimal. It’s much cheaper to catch a child before they fall into malnutrition than it is to treat them, not to mention the health benefits to the child from averting the disease. More work needs to be done to test and validate the most cost-effective prevention methods to ensure that only those that actually generate impact are scaled.
Childhood malnutrition sits at the intersection of public health and nutrition/agricultural programming. Current efforts are spread across the U.S. government and multilateral partners with little coordination toward desired outcomes. Funding that hypothetically targets childhood malnutrition can come from a variety of players in the U.S. government, ranging from Department of Defense to USAID to the Department of Agriculture. While some coordination through programs like Feed the Future exist at USAID, these programs are not yet results- or outcome-based. Coordination should involve measuring the impact of collective aid across agencies on an outcome like recovery rates or the number of children suffering from malnutrition in a given geographic area.
Investing in Digital Agriculture Innovation to Secure Food, Yields, and Livelihoods
Summary
Smallholder farmers and their households account for more than 2 billion people—almost one-third of humanity and more than two-thirds of the world’s poor. Smallholder farmers are the economic engine of local livelihoods and critical local sources of nutrition and food security. Their persistently low agricultural productivity is a major driver of global poverty and food insecurity. Many known agricultural practices and technologies could improve farmers’ yields and incomes, but systemic barriers and information gaps hamper their adoption. Today, with the rapid growth of mobile phone penetration throughout the developing world, we are in a unique moment to deploy new digital technologies and innovations to improve food security, yields, and livelihoods for 100 million smallholder farmers by 2030.
To spearhead USAID’s leadership in digital agriculture and create a global pipeline from tested innovation to scaled impact, USAID should launch a Digital Agriculture for Food Security Challenge, establish a Digital Agriculture Innovation Fund, and convene a Digital Agriculture Summit to jump-start the process.
Challenge and Opportunity
Two-thirds of the world’s ultra-poor depend on agriculture for their livelihood. Low productivity growth in this sector is the biggest obstacle to poverty reduction and sustainable food security. The Food and Agriculture Organization’s 2022 report on The State of Food Security and Nutrition in the World estimates that around 2.3 billion people—nearly 30% of the global population—were moderately or food insecure in 2021 and as many as 828 million were affected by hunger. Improving smallholder farmer incomes and local food security is critical to achieving the United Nations Sustainable Development Goals by 2030, particularly ending poverty (SDG 1) and eliminating hunger (SDG 2). Yet smallholder farmers typically harvest only 30%–50% of what they could produce. Smallholder farmers are particularly at risk from climate-driven shocks, and fundamental changes to growing conditions make climate adaptation a key challenge to improving and securing their yields.
More than $540 billion is spent in the agricultural sector each year through public budgets, mostly subsidies on farm inputs and outputs. Of USAID’s over $1 billion annual budget for agricultural aid, much attention is given to direct nutrition and economic assistance as well as institution and market-shaping programs. By contrast, efforts in climate adaptation and food security innovation like the Feed the Future Innovation Labs and Agriculture Innovation Mission for Climate (AIM for Climate) rely on traditional, centralized models of R&D funding that limit the entry and growth of new stakeholders and innovators. Not enough investment or attention is paid to productivity-enhancing, climate-adaptation-focused innovations and to translating R&D investment into sustainable interventions and scaled products to better serve smallholder farmers.
USAID recognizes both the challenge for global food security and the opportunity to advance economic security through evidence-driven, food-system level investments that are climate-driven and COVID-conscious. As directed by the Global Food Security Act of 2016, the U.S. Government Global Food Security Strategy (GFSS) 2022–2026 and its counterpart Global Food Security Research Strategy (GFSRS) highlight the potential for digital technologies to play a pivotal role in the U.S. government’s food system investments around the world. The GFSS describes “an ecosystem approach” that prioritizes the “financial viability of digital products and services, rather than one that is driven predominantly by individualized project needs without longer-term planning.” A core part of achieving this strategy is Feed the Future (FTF), the U.S. government’s multi-agency initiative focused on global hunger and food security. Administrator Samantha Powers has committed $5 billion over five years to expand FTF, creating an opportunity to catalyze and crowd in capital to build a thriving, sustainable global agriculture economy—including innovation in digital agriculture—that creates more resilient and efficient food systems.
However, USAID stakeholders are siloed and do not coordinate to deliver results and invest in proven solutions that can have scaled sustainable impact. The lack of coordination means potential digital-powered, impactful, and sustainable solutions are not fostered or grown to better serve USAID’s beneficiaries globally. USAID’s Bureau for Resilience and Food Security (RFS) works with partners to advance inclusive agriculture-led growth, resilience, nutrition, water security, sanitation, and hygiene in priority countries to help them accelerate and protect development progress. USAID’s FY 2023 budget request also highlights RFS’s continued focus on supporting “partner countries to scale up their adaptation capacity and enhance the overall climate resilience of development programming.” The FTF Innovation Labs focus on advanced agricultural R&D at U.S. universities but do not engage directly in scaling promising innovations or investing in non-academic innovators and entrepreneurs to test and refine user-centered solutions that fall within FTF’s mandate. USAID’s emerging Digital Strategy and Digital Development Team includes specific implementation initiatives, such as a Digital Ecosystem Fund and an upcoming Digital Vision for each sector, including agriculture. USAID is also planning to hire Digital Development Advisors, whose scope aligns closely with this initiative but will require intentional integration with existing efforts. Furthermore, USAID country missions, where many of these programs are funded, often do not have enough input in designing agriculture RFPs to incorporate the latest proven solutions and digital technologies, making it harder to implement and innovate within contract obligations.
This renewed strategic focus on food security through improved local agricultural yields and climate-resilient smallholder farmer livelihoods, along with an integration of digital best practices, presents an opportunity for USAID and Feed the Future. By using innovative approaches to digital agriculture, FTF can expand its impact and meet efficiency and resilience standards, currently proposed in the 2022 reauthorization of the Global Food Security Act. While many known agricultural practices, inputs, and technologies could improve smallholder farmers’ yields and incomes, adoption remains low due to structural barriers, farmers’ lack of information, and limitations from existing agriculture development aid practices that prioritize programs over sustainable agricultural productivity growth. Today, with the rapid pace of mobile phone penetration (ranging between 50% and 95% throughout the developing world), we are in a unique moment to deploy novel, emerging digital technologies, and innovations to improve food security, yields, and livelihoods for 100 million smallholder farmers by 2030.
There are many digital agriculture innovations – for example digital agricultural advisory services (DAAS, detailed below) – in various stages of development that require additional investment in R&D. These innovations could be implemented either together with DAAS or as stand-alone interventions. For example, smallholder farmers need access to accurate, reliable weather forecasts. Weather forecasts are available in low- and middle-income countries (LMICs), but additional work is needed to customize and localize them to farmers’ needs and to communicate probabilistic forecasts so farmers can easily understand, interpret, and incorporate them in their decision-making.
Similarly, digital innovations are in development to improve farmers’ linkages to input markets, output markets, and financial services—for example, by facilitating e-subsidies and mobile ordering and payment for agricultural inputs, helping farmers aggregate into farmer producer organizations and negotiate prices from crop offtakers, and linking farmers with providers of loans and other financial services to increase their investment in productive assets.
Digital technologies can also be leveraged to mobilize smallholder farmers to contribute to climate mitigation by using remote sensing technology to monitor climate-related outcomes such as soil organic carbon sequestration and digitally enrolling farmers in carbon credit payment schemes to help them earn compensation for the climate impact of their sustainable farming practices.
| Digital agricultural advisory services (DAAS) leverage the rapid proliferation of mobile phones, behavioral science, and human-centered design to build public extension system capacity to empower smallholder farmers with cutting-edge, productivity-enhancing agricultural knowledge that improves their food security and climate resilience through behavior change. It is a proven, cost-effective, and shovel-ready innovation that can improve the resilience of food systems and increase farmer yields and incomes by modernizing the agricultural extension system, at a fraction of the cost and an order of magnitude higher reach than traditional extension approaches. DAAS gives smallholder farmers access to on-demand, customized, and evidence-based agricultural information via mobile phones, cheaply at $1–$2 per farmer per year. It can be rapidly scaled up to reach more than a hundred million users by 2030, leading to an estimated $1 billion increase in additional farmer income per year. USAID currently spends over $1 billion on agricultural aid annually, and only a small fraction of this is directed to agricultural extension and training. Funding is often program-specific without a consistent strategy that can be replicated or scaled beyond the original geography and timeframe. Reallocating a share of this funding to DAAS would help the agency achieve strategic climate and equity global food security goals. Scaling up DAAS could improve productivity and transform the role of LMIC government agricultural extension agents by freeing up resources and providing rapid feedback and data collection. Agents could refocus on enrolling farmers, providing specialized advice, and improving the relevance of advice farmers receive. DAAS could also be integrated into broader agricultural development programs, such as FAO’s input e-subsidy programs in Zambia and Kenya. |
Plan of Action
To spearhead USAID’s leadership in digital agriculture and create a global pipeline from tested innovation to scaled impact, USAID, Feed the Future, and its U.S. government partners should launch a Digital Agriculture for Food Security Challenge. With an international call to action, USAID can galvanize R&D and investment for the next generation of digitally enabled technologies and solutions to secure yields and livelihoods for one hundred million smallholder farmers by 2030. This digital agriculture moonshot would consist of the following short- and long-term actions:
Recommendation 1: Allocate $150 million over five years to kickstart the Digital Agriculture Innovations Fund (DAI Fund) to fund, support, and scale novel solutions that use technology to equitably secure yields, food security, and livelihoods for smallholder farmers.
The fund’s activities should target the following:
- Digital Agriculture Pilot and Research Fund (DAPR Fund) ($35 million): Provide funding for research, user design, and pilot testing to industry, NGO, and university innovators to create and verify digital innovations like customized weather forecasts, digital extension, microinsurance, microcredit, and local input dealer directories. This could employ the Small Business Innovation Research model and use technical assistance from within the agency and in partner organizations to support the development of promising new ventures or products/services from existing players.
- Digital Agriculture Scaling and Commercialization Fund ($100 million): Invest in grants or, with collaboration from U.S. International Development Finance Corporation, in equity funding for proven digital agriculture solutions as bridge capital to enhance their scaling to new markets or products. Funding should be directed not only to FTF Innovation Labs solutions but also to those outside the FTF network with a focus on LMIC-founded ventures, digital and technology-enabled startups, and existing footprints in FTF target countries to ensure broader impact. Selected solutions should have demonstrated outcomes in proof of concept and moved into the “demonstrated uptake” phase of the product life cycle. Annual investments should be up to $10 million across a small portfolio of ventures to crowd-in unlocked private capital and foster competitive, sustainable enterprises. Contract authority should be flexible and mission-oriented.
- Market-Shaping and Public-Private Partnerships ($15 million): Create an Advanced Research Projects Agency-Energy (ARPA-E) style Tech-to-Market Team, a separate group of staffers working full-time to find marketing opportunities for novel technologies in the innovation pipeline. This group could coordinate new public-private partnerships, like the Nutritious Foods Financing Facility (N3F), which can support the digital agriculture ecosystem for smallholder farmers. This funding would also allow for the hiring of a cadre of dedicated digital development advisors at USAID to spearhead this work in the digital agriculture sector and collaborate with agency country missions in planning and executing RFPs and other agricultural aid programs.
The fund’s investment priorities should align with stated GFSS and GFSRS objectives, including solutions focused on climate-smart agricultural innovation, enhanced nutrition, and food systems, genetic innovation, and poverty reduction. Program activities and funding should coordinate with FTF implementation in strategic priority countries with large agricultural sectors and mature, low-cost mobile networks such as Ethiopia, India, Kenya, Nigeria, and Pakistan. It should also collaborate with the FTF Innovation Lab and the AIM for Climate Initiative networks.
Recommendation 2: Convene the Digital Agriculture Summit to create an all-hands-on-deck approach to facilitate and accelerate integrated digital agriculture products and services that increase yields and resilience.
USAID will announce the dedicated DAI Fund, convening its interagency partners—like the US Department of Agriculture (USDA), Development Finance Corporation (DFC), Millennium Challenge Corporation (MCC), US Africa Development Foundation (USADF) as well as philanthropy, private sector capital, and partner country officials and leaders to chart these pathways and create opportunities for collaboration between sectors. The Summit can foster a community of expertise and solidify commitments for funding, in-kind resources, and FTF country partnerships that will enable DAI Fund solutions to demonstrate impact and scale. The Summit could occur on the sidelines of the United Nations General Assembly to allow for greater participation and collaboration with FTF country representatives and innovators. Follow-up activities should include:
- Partner Country Commitments: Secure commitments from FTF partner countries to direct annual funding toward digital infrastructure and the development of a local digital agriculture economy, whether in the form of R&D, implementation, or infrastructure funding.
- Philanthropic and Private Sector Commitments: Following the Grand Challenges model, the Digital Agriculture for Food Security Challenge should seek commitments from philanthropy and private sector funders to expand the funding pool and finance pipelines for startups. Invitation to the Summit would be contingent on commitments of financial support and in-kind resources for digital agriculture innovation.
- SXSAg for Digital Agriculture: Annual gatherings of innovators, investors, and stakeholders to share knowledge and results as well as attract more private capital.
- Innovator Community of Practice: Create a Community of Practice of innovators and experts inside and outside the agency to advise DAI Fund staff and USAID on current challenges in the digital agriculture space for non-established entrants and opportunities for future fund investments.
- Webinar Series: As a follow-up to the Summit, a webinar series could disseminate knowledge and build institutional buy-in and support for DAAS with key stakeholders within the agency. Subject matter experts from PxD and other service providers can share evidence, use cases, and lessons learned in developing and delivering these services and provide recommendations on how USAID can better incorporate digital agriculture into its operations.
Conclusion
With the exponential adoption of mobile phones among smallholder farmers in the past decade, digital agriculture innovations are emerging as catalytic tools for impact at an unprecedented scale and social return on investment. Devoting a small percentage (~2%–5%) of USAID’s agricultural aid budget to DAAS and other digital agriculture innovations could catalyze $1 billion worth of increased yields among 100 million smallholder farmers every year, at a fraction of the cost and an order of magnitude higher reach than traditional extension approaches.
Achieving this progress requires a shift in strategy and an openness to experimentation. We recommend establishing a Digital Agriculture Innovation Fund to catalyze investment from USAID and other stakeholders and convening a global Digital Agriculture Summit to bring together subject matter experts, USAID, funders, and LMIC governments to secure commitments. From our experience at PxD, one of the world’s leading innovators in the digital agriculture sector, we see this as a prime opportunity for USAID to invest in sustainable agricultural production systems to feed the world and power local economic development for marginalized, food-insecure smallholder farmers around the world.
More from Jonathan Lehe, Gautam Bastian, and Nick Milne can be found at Precision Development.
Using the reach and power of the US government and its leaders as a platform to convene, multi-sector stakeholders can be brought together to outline a common agenda, align on specific targets, and seek commitments from the private sector and other anchor institutions to spur collective, transformational change on a wide range of issues aligned to the goals and interests of the federal agency and Administration’s priorities. External organizations respond to these calls-to-action, often leading to the development of partnerships (formal and informal), grand challenges, and the building of new coalitions to make financial and in-kind commitments that are aligned with achieving the federal government’s goals. A commitment could be modeled after how the State Department’s convened the Global Alliance for Clean Cookstoves:
- a financial contribution (e.g.) the U.S. pledged nearly $51 million to ensure that the Global Alliance for Clean Cookstoves reaches its ‘100 by 20,’ which calls for 100 million homes to adopt clean and efficient stoves and fuels by 2020.
- shared expertise: the organization mobilizes experts in a variety of issues: gender, health, security, economics, and climate change to address significant risk factors. The U.S. will also offer assistance to implement cookstoves.
- research and development: the U.S. is committed to an applied research and development effort that will serve as the backbone of future efforts in the field that includes analyzing health and environmental benefits of using clean stoves, developing sustainable technologies, and conducting monitoring to ensure success of the Alliance’s goals.
USAID is a leader in the US government in running open innovation challenges and prizes. Other U.S. government agencies, foreign government aid agencies, and philanthropies have also validated the potential of open innovation models, particularly for technology-enabled solutions. USAID’s Grand Challenges for Development (GCDs) are effective programmatic frameworks that focus global attention and resources on specific, well-defined international development problems and promote the innovative approaches, processes, and solutions to solving them.
Conceived, launched, and implemented in coordination with public and private sector partners, Grand Challenges for Development (see list below) emphasize the engagement of non-traditional solvers around critical development problems. The Grand Challenges for Development approach is a complement to USAID’s current programming methods, with each GCD is led by experts at the bureau level. These experts work directly with partners to implement the day-to-day activities of the program. The Grand Challenges for Development programs show how the power of the framework can be leveraged through a variety of modalities, including partnerships, prizes, challenge grant funding, crowdsourcing, hack-a-thons, ideation, and commitments. The Digital Agriculture for Food Security Challenge could mimic a GCD program like Saving Lives at Birth by providing consistent funding, resources, and energy toward new meaningful, cost-effective breakthroughs to improve lives where solutions are most needed.
Information provision, including DAAS, is a difficult product for private sector entities to deliver with a sustainable business model, particularly for smallholder farmers. The ability and willingness to pay for such services is often low among resource-poor smallholder farmers, and information is easily shareable, so it is hard to monetize. National or local governments, on the other hand, have an interest in implementing digital solutions to complement in-person agricultural extension programs and subsidies but tend to lack the technical capacity and experience to develop and deliver digital tools at scale.
USAID has the technical and institutional capacity to provide digital agriculture services across its programs. It has invested hundreds of millions of dollars in agricultural extension services over the past 60 years and has gained a strong working knowledge of what works (and what doesn’t). Digital tools can also achieve economies of scale for cost relative to traditional in-person agriculture solutions. For instance, in-person extension requires many expenses that do not decrease with scale, including fuel, transportation, training, and most importantly the paid time of extension agents.
One estimate is that extension agents cost $4,000 to $6,000 per year in low-income countries and can reach between 1,000 to 2,000 farmers each—well above the World Bank recommended threshold of 500 farmers per agent—bringing annual costs to $2–$6 per farmer per year. This estimate assumes a farmer-to-agent ratio well above the World Bank’s recommended threshold of 500:1. In other contexts, it has been estimated as high as $115. We estimate a cost-effectiveness of $10 in increased farmer income for every $1 invested in programs like DAAS, which is an effective return on American foreign development assistance.
Digital solutions require not only the up-front cost of development and testing but also maintenance and upkeep to maintain effectiveness. Scaling these solutions and sustaining impact requires engaged public-private partnerships to reduce costs for smallholder famers while still providing positive impact. Scaling also requires private capital – particularly for new technologies to support diffusion and adaptation – but is only unlocked by de-risking investments by leveraging development aid.
As an example, PxD engages directly with national governments to encourage adoption of DAAS, focusing on building capacity, training government staff, and turning over systems to governments to finance the operation and maintenance of systems into perpetuity (or with continued donor support if necessary). For instance, the State Government of Odisha in India built a DAAS platform with co-financing from the government and a private foundation, scaled the platform to 3 million farmers, and transitioned it to the government in early 2022. A similar approach could support scale across other geographies—especially given USAID’s long-standing relationships with governments and ministries of agriculture.
A growing body of evidence shows that DAAS can have a significant impact on farmers’ yields and incomes. Precision Development (PxD) currently reaches more than 7 million smallholder farming households with DAAS in nine countries in Africa, Asia, and Latin America, and there is a well-established market with many other service providers also providing similar services. This research, including several randomized control trials conducted by PxD researchers in multiple contexts as well as additional research conducted by other organizations, shows that DAAS can improve farmer yields by 4% on average in a single year, with benefit-cost ratios of 10:1, and the potential for these impacts to increase over time to create larger gains.
There is also evidence of a larger impact in certain geographies and for certain crops and livestock value chains, as well as a larger impact for the subset of farmers who use DAAS the most and adopt its recommendations.
What we learned in Mexico City
Moonshots seem impossible—until they’ve hit their target. This was the mantra of our in-person accelerator workshop, hosted with our partners at Unlock Aid in Mexico City. The workshop was just one part of our larger accelerator process where we’re working with innovators to develop moonshots around global development targets. FAS’s largest policy-development convening to date brought together over 70 participants (representing 40+ organizations, 25+ countries, and six continents) to think through creative approaches for achieving the United Nations Sustainable Development Goals by 2030.

After years of Zoom calls, phone conferences, and emails, meeting our accelerator cohort in person was a refreshing change of pace. Connecting IRL enabled free-flowing collaboration on big issues like global water security, access, and safety. We saw convergence across organizations: City Taps, Drinkwell, and Evidence Action came together to create the “WaterShot”—a new approach to solving water access with an outcomes marketplace framework. We were reminded anew that policy is powered by people—and that strong interpersonal connections inevitably lead to better and more creative policy ideas.
Brainstorming at the event was inspired by remarks from global development leaders. Project Drawdown spoke about the Drawdown Framework for climate solutions, NPX Advisors demonstrated how to drive better outcomes with advanced market commitments, and Nasra Ismail, a leader in global development strategy, talked about the power of coalition building.

The workshop was an initial opportunity to expose global development experts to the idea that policy, like seed funding or infrastructure investment, is an input that supports scaling. Most individual innovators are understandably hyper-focused on scaling up their individual ideas or products. But good policy is needed to build a flourishing global development environment—a rising tide that lifts all entrepreneurial ships. An underlying theme of the Mexico City workshop was the importance of policy as a growth enabler.
Now that we’re back in DC and over our jetlag, the accelerator continues, and we’re working with workshop participants to inform policymakers on key priorities for global development policy. We’re thinking about pain points in the field and opportunities for systems change, including earmarking funds for innovation, uplifting and incorporating community voices to policy, and setting new standards that focus on results.
The field of global development can be individualized and competitive—grants are few and far between, which doesn’t always foster shared best practices. But achieving the SDGs by 2030 must be a collaborative effort. Problems like climate change and food security are more pressing than ever, and they require an entirely new way of thinking about global development—finding and building on opportunities from proven results. Later this fall, look out for our participants’ moonshot memos as we roll them out. And if you have an idea about meeting the SDGs with a moonshot—or something else—why not submit it? Aiming at the moon is one thing, but getting there takes dedicated and sustained collaboration, and we’re so honored that these daring organizations want to work with us to do just that.

The Day One Project is going international!
The Day One Project is going international! My colleague Josh Schoop and I will be spending this week in Mexico City with our partners at Unlock Aid, where we’ll be co-hosting the Reimagining the Future of Global Development Moonshot Accelerator. This will be our eighth accelerator cohort, and the very first in-person group.
We’re convening a group of 70 entrepreneurs, innovators, policymakers, and funders from around the world to think big about the future of global development and how government, business, industry, and aid can meet the UN’s Sustainable Development Goals (SDGs) by 2030. With the recent passage of a historic investment in the transition away from fossil fuels, the time is now to act on the biggest threats facing humanity. Sitting squarely within ‘the decade of delivery’—the remaining years we have to achieve the SDGs— this moonshot accelerator serves as an important call for action.
Our goal for this accelerator is to disrupt. We aim to generate new models to seed, scale, and implement catalytic solutions. The inspiration for the design of this accelerator comes from the “moonshot” model that the Kennedy administration pioneered to put the first man on the moon. A moonshot has since come to mean solving a daunting problem in an accelerated time period, requiring breakthrough, innovative, and radical thinking. If the past decades have not delivered the necessary change, then we have to shoot for the moon.
Over the course of the week, we’ll be working with the accelerator cohort to develop their own moonshots in health, the green economy, biodiversity, food and water insecurity, and more. These moonshots will be the building blocks for a Global Development Outcomes Marketplace, pitching funders and policymakers on new ways to unlock innovation in global development. Innovation here involves so much more than just new technology – it means new systems, processes, cooperation, organizing, and change, while ensuring that diverse perspectives are leading the way forward.
We’re really invested in these ideas and the people driving them, so here’s a sneak peek at a couple innovative groups joining us in Mexico City: Instiglio, headquartered in Bogotá, Colombia, is experimenting with new global development systems, like innovative financing methods, while SwipeRx in Indonesia is dedicated to revolutionizing the pharmacy industry with a tech-based solution. There are, of course, so many more groups who’ll be discussing and testing their ideas in-person, and the goal is to channel this cohort’s diverse expertise to create high-level, actionable recommendations for funders and multilateral organizations that center equity and outcomes.
I’m most excited to hear from experts and entrepreneurs from all over the world on what has been holding back progress despite attempted solutions, and I look forward to collaborating on what a new set of systems could look like. I’m excited to learn from our inspiring cohort, and to build mutual understanding across sectors to find ways to improve current solutions and break ground on a new path forward.I have high hopes that this accelerator will reinvigorate global development and uplift new voices and ideas in order to build a more prosperous planet. I resonate strongly with the voices of young people demanding urgent climate action worldwide–it’s time to harness this momentum to make sustainable, transformative change. Follow the journey of our first in-person accelerator on Twitter.
Accelerating Innovation, Performance, and Impact at USAID
Summary
The United States Agency for International Development (USAID) tackles some of the toughest challenges in some of the toughest places on earth, including fighting global pandemics, growing economic prosperity, strengthening democratic institutions, and providing humanitarian relief. USAID plays an important role in addressing global development problems that initially lack effective, scalable, and sustainable solutions. Yet USAID’s activities allow little room for the risk taking or iteration needed to drive significant improvements and encourage disruptive new ideas, with most programs implemented through detailed plans with rigid designs.
Imagine if the pace of progress for global development could match the breakneck pace of advances in the tech sector. The next administration should assess where current USAID interventions are inadequately meeting global need, applying best practices from innovation to improve programs accordingly. This will include shifting to outcomes-based performance metrics, dedicating budget for experimentation, establishing incentives that encourage risk-taking, linking payments with outcomes, and conducting ex-post evaluations of scale and sustainability.
Energy and World Economic Growth
Introduction
Rapid growth in the developing world has changed the economic center of gravity towards Asia, especially with regard to the world’s energy economy. World-wide demand for energy, especially energy that can propel automobiles, is increasing. High energy growth is producing two problems. The first, widely recognized, is the increased greenhouse gas concentrations that result from burning fossil fuels. Barring a substantial reduction of fossil fuel use, world-wide temperatures could increase to dangerous levels. While the huge infrastructure of the energy economy rules out quick changes, if action is taken now, the necessary world-wide reduction of greenhouse gas emissions may still be possible. However, the required uptake of clean energy technologies will require strong government policies to offset initial investment costs.1
The second problem is less widely recognized. The share of GDP that must be spent on oil supplies may also limit economic growth. At times, the price of oil is limited only by the strain it places on the world economy. We have seen episodes where high and rising oil prices precede an economic downturn. During the downturn, oil prices can drop to levels that, along with a weak economy, discourage investment in new oil production. When strong growth returns, we can see the cycle repeated.
These events are not surprising because oil has a very low elasticity of demand and supply with respect to price. That means very large price changes are required to increase supply or decrease demand. In addition, oil has a very high elasticity of demand with respect to income. That means economic growth strongly increases oil demand. Lastly, oil expenditures can be a large enough component of GDP to adversely affect economic growth if they grow too large. Added together, these interactions can produce the following cycle:
- High GDP growth drives oil prices to high levels since high income elasticity increases oil demand while low price elasticities require high oil prices to balance demand and supply2;
- The resulting high share of GDP spent on oil reverses GDP growth;
- With lower GDP growth, high income elasticity reduces oil demand;
- With lower oil demand, low oil price elasticities sharply lower oil prices; and
- Low oil prices reduce oil production investments but encourage high GDP growth.
Oil prices are only one factor affecting the world economy. Nonetheless, world GDP growth and oil prices are periodically engaged in the cycle described above. Oil prices can also stabilize at levels that are not high enough to cause a downturn in GDP growth, while GDP growth is not high enough to push oil prices past the level where the share of GDP spent on oil reverses GDP growth.3
The Clean Energy Challenge
High economic growth encourages more fossil fuel use and increased greenhouse gas concentrations. High oil prices also provide an opportunity for clean alternatives to be more competitive. However, if high oil prices periodically blunt economic growth, it is more difficult to make clean-energy policies a government priority. Economies that are struggling with low growth and high unemployment are less likely to maintain strong clean-energy policies. Without these policies, we cannot hope to limit the increase of world-wide temperatures to 2oC above pre-industrial levels, the level deemed likely to avoid the more serious consequences of climate change and accepted by the G8 countries as a target to be achieved by international climate policies.4
A recent IEA study5 estimated the increase in clean power-sector technologies that would be needed to prevent a world-wide temperature increase of over 2oC (Figure 1). They estimate that the future annual growth of nuclear power must be between 23 and 31 gigawatts (GW). To put this into perspective, the historic high in building nuclear power plants was 27 gigawatts per year (GW/yr). Photovoltaic power must, after 2020, reach 50 GW/yr and, after 2030, exceed 100 GW/yr. Onshore wind investments must exceed 60 GW/yr from now through 2050. Offshore wind must exceed 20 GW/yr after 2020. After 2020, coal with carbon capture and storage would need to grow by more than 20 GW/yr.
The challenges to achieving the 2oC scenario in the transport sector are no less daunting, requiring that the world sales of electric vehicles double each year between 2012 and 2020. Advanced biofuel production must grow from ~ zero to 22 billion gallons by 2020. IEA estimates that the incremental energy-sector investment that would be needed to keep world-wide temperatures from increasing over 2oC is $37 trillion (cumulative investment between now and 2050).6 The bulk of this investment would have to be made in the developing world. It is not likely that these additional investments, over and above what is necessary to provide required energy supplies, will be made without strong government policies, even though they would produce offsetting savings in the long term. Without strong world-wide economic growth, it will be difficult, if not impossible, to implement the policies necessary to achieve the 2oC scenario.
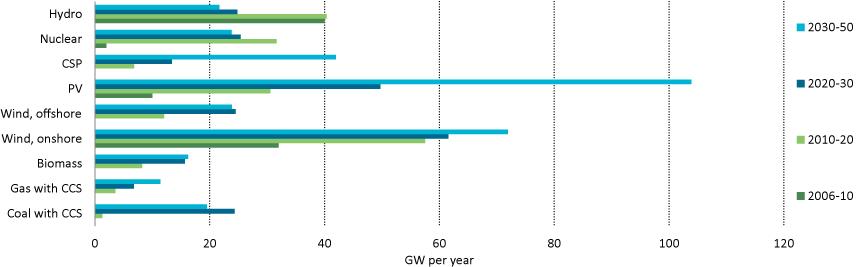
Average Annual Electricity Capacity Additions to 2050
2012 IEA Energy Technology Perspectives 2oC Scenario
Source: IEA, Energy Technology Perspectives 2012
Oil and Economic Growth
World oil prices have, from time to time, reached levels that have impaired world economic growth such as the aftermath of the 1973 oil embargo. This first “energy crisis” accompanied a major change in the way petroleum was controlled and priced. Prior to 1970, world oil prices were managed by a relatively small number of large oil companies. These companies enjoyed liberal access to most countries’ oil resources. They could develop large oil fields in host countries with terms that allowed ample world supply at non-competitive but reasonable prices. These companies pursued a strategy to maintain affordable and stable oil prices that supported economic growth in the industrialized world and encouraged increased demand for oil. These arrangements were undone by reforms in the member-countries of the Organization of Petroleum Exporting Countries (OPEC). The reforms moved the control of the world’s largest oil resources from the international oil companies to OPEC and, given sufficient OPEC cohesion, the ability to control of world oil prices. OPEC’s control of oil prices was short-lived. The rapid price hikes associated with the 1973 embargo and the 1979 Iranian revolution stimulated new supplies, especially from the North Sea and Alaska. High oil prices also stymied demand as consumers turned to more efficient automobiles.
By 1981, oil prices began a steady decline. Saudi Arabia tried to maintain higher prices by cutting production until by 1985, its output had fallen to 3 million barrels per day (mmb/d), 70 percent lower than it had been in 1980. In 1986, Saudi Arabia adopted netback pricing7 to regain market share. Oil prices collapsed to $10 per barrel (/b)8. By 1988, the OPEC pricing regime was replaced by commodity market pricing, a system that remains in place today and for the foreseeable future. The London InterContinental Exchange (ICE) established a contract for Brent, a mixture of high quality North Sea crudes[ref]The selection of Brent and WTI as marker crudes reflected several factors: 1) the desirability of Brent and WTI to most refiners; 2) the sources of Brent (UK and Norway) and WTI (United States) relative to the world’s financial capitals, London and New York; 3) the supply of Brent and WTI would not be controlled by national governments or OPEC; and 4) Brent and WTI were produced in sufficient volume to be an important component of world oil supply.[/ref]. Additionally, the New York Merchantville Exchange (NYMEX) established a contract for West Texas Intermediate (WTI), high-quality crude similar to Brent.
Only a small percentage of the world’s crude petroleum is WTI, Brent or other traded crudes. Nonetheless, these marker crudes affect the contract price of other types of crude oil since most crude oil contracts are indexed to one or more marker crudes. Spot oil prices also respond to whether the oil commodity markets are in backwardation or contango9
This new pricing regime did not entirely eliminate OPEC’s price setting role. A few OPEC countries maintain spare production capacity. Saudi Arabia, by far, keeps the largest production capacity in reserve. Saudi Arabia can increase or decrease its oil production in response to world market conditions. If Saudi Arabia believes that prices are too high, they can put spare capacity into production, putting downward pressure on market prices. Likewise, if Saudi Arabia believes that prices are too low, they can reduce production (increasing spare capacity) putting upward pressure on market prices. Most other oil producing countries and all private oil companies are price takers. They only respond to higher or lower oil prices by increasing or decreasing planned investments in new production capacity. Whether or not these investments are made has little impact on current oil supplies or prices, but has a large impact on future oil supplies and prices.
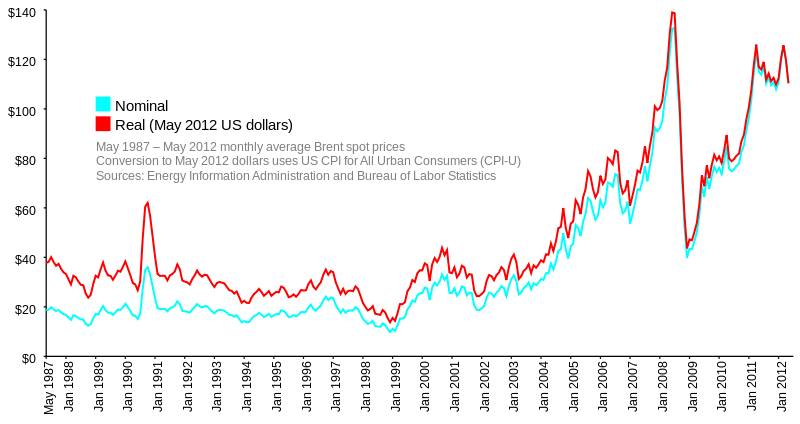
The new pricing regime produced relatively stable oil prices until 1999 (except for a sharp increase in 1990 due to the Gulf War). In 1999, oil prices began a sharp upward trend culminating in an extremely sharp $40/b rise from January 2007 to June 2008. With record high oil prices, U.S. demand finally slackened and, soon after, failing financial institutions launched a world-wide banking crisis. Oil prices plummeted reversing in one year the gains made since 2005.
Since 2008 there have been two rapid increases in oil prices. In early 2011, the Libyan civil war removed 1.5 mmb/d of light-sweet crude from the market. Oil prices spiked again in 2012 due to increased supply outages from Iran, Nigeria, Sudan and Yemen. The 2012 run-up was followed by a significant price slide due to a deteriorating economic outlook in the Eurozone and uncertainty whether the EU and the European Central Bank would take the necessary actions to prevent an unraveling of the euro.
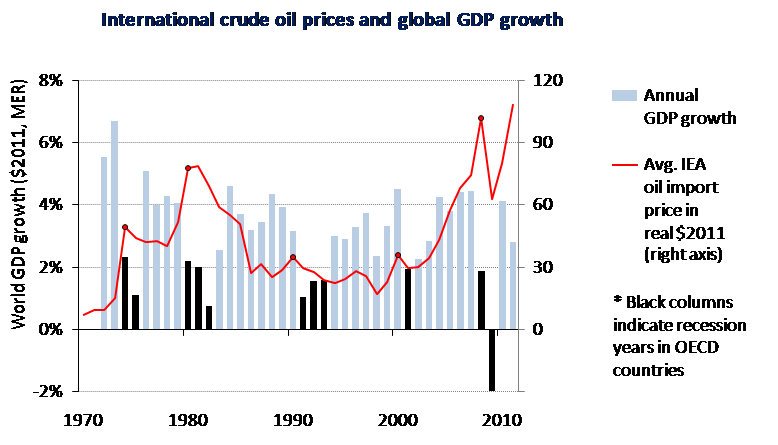
Source: IEA, World Energy Outlook 2011
Figure 3 shows oil prices and annual changes in world-GDP. Each spike in oil prices was followed by a sharp drop in world GDP growth. The price rise from the 1973 oil embargo preceded a 4% drop in world GPD growth. Within two years, world growth slid from over 6% to 1%. The oil-supply outage resulting from the 1979 Iranian revolution doubled oil prices. Growth slid from 4% to 2% and, later, to below 1%.
The spike in oil prices resulting from the 1990 Gulf War led to a drop in world GDP growth from over 3% in 1990 to 1% in 1991. GDP growth did not reach 3% until 1994. The price spike from 1999-2000 was followed by a drop in world GDP growth from over 4% in 2000 to 2% in 2001. The world economy appeared to survive the long price rise from 2002 to 2007 until 2008, when the world suffered the worst financial crisis since the 1930s. World GDP growth dropped from over 4% in 2007, declined to less than 2% in 2008 and plummeted to -2% in 2009. While these high oil prices did not cause the world-wide recession, they were a contributing factor. High oil prices directly affected automobile sales and travel-related industries. High oil prices also reduced a household’s disposable income for other goods and services that remained after paying unavoidable fuel expenses.10
While each oil spike has been followed by a sharp drop in world economic growth, since 198711, there has been only one sharp reduction in world economic growth that was not preceded by an oil price spike.12 GDP growth has remained above 3%, apart from the 2nd or 3rd years following an oil price spike.
The world oil market has been subject to unplanned supply outages for quite some time. However, since 2011, supply outages have increased considerably from most prior years. They also reflect causes are likely to be chronic conditions as opposed to one-off events. During 2010, oil supply outages averaged less than 1 mmb/d; since 2011, they have averaged ~ 3 mmb/d and remain high today. Reports of insurgent attacks on oil-producing and distribution infrastructure, ethnic or sectarian conflict and civil war in the oil-producing states of the Middle East and North Africa (MENA) are too common to enumerate. The security situation has caused private industry to withdraw personnel from regions that are not deemed to be safe. In addition to loss of trained personnel, insurgent attacks on infrastructure, political disputes concerning sovereignty, disagreements about the validity of oil-related contracts and other problems are not likely to be passing problems that we can assume will be resolved. While these may be necessary side effects as countries replace autocratic rule with democratic governments, they nonetheless pose a great risk for future oil supplies. The International Energy Agency recently warned that relatively stable oil prices should not conceal “an abundance of risk” as “much of the Middle East and North Africa remains in turmoil.” “The current stalemate between the West and Iran” is “unsustainable” and “sooner or later, something has to give.” The political situation in the MENA region reflects a “precarious balance” that does not bode well for “clear, stable and predictable oil policies, let alone supplies.”13
OPEC production capacity has been essentially flat for the last 30 years. Over that time, growing oil demand has been met by additions to non-OPEC capacity. A number of disappointing non-OPEC supply developments helped drive the sharp rise in oil prices from 2002 and 2008. During that period, the cost of oil and gas drilling equipment and support activities increased by 260%.14 More recently, the growth of Canadian oil sands and U.S. tight oil production has kept the world oil market in balance. Without increased oil production in the United States and Canada, non-OPEC production would have been in decline in recent years.
Sufficiently high oil prices are needed to sustain the growth on non-OPEC oil. The IEA estimates that the cost of oil sands and tight oil production ranges from $45/b to over $100/b. 15 As production moves from the most productive plays to less promising plays, costs will tend to move to the upper end of the IEA range. For example, Global Energy Securities estimates that the price of oil needed to generate an attractive internal rate of return increases from $67/b in Eagle Ford (Texas) to $84/b in Monterey/Santos (California).16 While current oil prices are higher than they need to be to justify increased investment, they are not that much higher than what’s needed to motivate the large investments needed to grow non-OPEC oil production.17
As long as world oil demand grows, so will the cost of oil. The only long-term pathway to lower oil prices is to reduce and reverse the growth of world oil demand.
World Economic Growth, Unemployment and Poverty
In OECD 18 economies, unemployment is the most serious consequence of limited GDP growth. Okun’s law describes a statistical relationship between an economy’s potential rate of growth, its actual rate of growth and changes in unemployment. According to this rough relationship, a 2% difference between a country’s actual GDP and its potential is associated with 1% more unemployment. Applied over time, unemployment will grow by 1% if economic growth is 2% below an economy’s potential.19 The picture in developing countries is more complicated because of movements of labor between the agricultural and industrialized economies. Growth below a developing country’s economic potential limits or reverses the movement from the agricultural sector to the industrial sector causing underemployment.20
While increasing productivity within the agricultural sector is a development priority, it also leads to underemployment in the agricultural sector.
The relationship between economic growth and the movement of the population out of the agricultural sector is vividly illustrated in the recent history of China. By the late 1970s China possessed an inefficient agricultural economy with a rudimentary industrial sector. China possessed a population exceeding 1 billion people, of which the vast majority lived in poverty. Economic reforms produced a sustained GDP growth that has averaged 10.2 percent per year.21As a result, China has moved 400 million people out of poverty into the modern economy. Currently, ~ 650 million people still live in the agricultural sector, 450 million more people than are needed.
High Chinese economic growth would permit more people to move out of the underemployed agricultural economy to productive labor in the modern economy, as there are 450 million people living in poverty.22 Within one generation, emigration out of the agricultural sector can be the first step to careers in commerce, business, education, medicine, engineering, science and management.
Reducing Petroleum Demand
By 2014, more oil will be consumed outside the OECD than within.23 Increased personal income and increased auto ownership appear to be as inextricably linked in rapidly developing economies as it had been in the OECD after the Second World War. With economic growth, automobiles (especially luxurious automobiles), are likely to be purchased in increasing numbers. Domestic automobile consumption will also help developing economies move from export reliance to supplying domestic markets.
With a rapidly increasing consumption of energy for personal mobility, it is imperative to satisfy this growth with non-petroleum energy. If the world continues to rely on petroleum fuels for personal mobility, high oil prices are likely to cause periodic episodes of low growth causing significant hardships for hundreds of millions of people.
Energy Security Trust
The Energy Security Trust, proposed by President Obama,24 aims to make current electric vehicle technologies cheaper and better with $2 billion for research. In addition to advances in batteries, electric vehicles and ubiquitous electric refueling, it will also fund sustainable biofuels.25 As stated by the White House; “In each of the last four years, domestic production of oil and gas has gone up and our use of foreign oil has gone down. And while America uses less foreign oil now than we’ve used in almost two decades, there’s more work to do. That’s why we need to keep reaching for greater energy security. And that’s why we must keep developing new energy supplies and new technologies that use less oil. The Secure Energy Trust will ensure American scientists and research labs have the support they need to keep our country competitive and create the jobs of the future.” The success of initiatives like the Energy Trust Fund would produce world-wide benefits as the uptake of competitive advanced clean energy technologies would be global. Competitive alternatives to petroleum-fueled personal transportation, combined with strong clean-energy policies, would go a long way to achieving the G8’s 2oC climate goal. They would also remedy an important impediment to world GDP growth.
Carmine Difiglio is the Deputy Assistant Secretary for Policy Analysis, U.S. Department of Energy and may be reached at carmine.difiglio@hq.doe.gov. His work and publications include the first engineering-economic transportation-energy model, several other modeling projects including the International Energy Agency’s Energy Technology Perspectives project, studies of international oil and natural gas markets, and policies to promote energy security, energy efficiency, motor-vehicle efficiency and alternative transportation fuels. Difiglio also serves as Co-Chair of the World Federation of Scientists’ Permanent Monitoring Panel on Energy and Vice-Chair of the IEA Standing Group on the Oil Market. He was Vice-Chair of the IEA Committee on Energy Research and Technology, Chairman of the IEA Energy Efficiency Working Party and Chairman of the Transportation Research Board Committee on Energy and Transportation. Difiglio’s Ph.D. is from the University of Pennsylvania. The data and views expressed in this paper are those of the author and are not endorsed by the U.S. Department of Energy or the United States government.