Prepared under the auspices of Karen Monaghan, Acting National Intelligence Officer for Economics and Global Issues.
Additional copies of this assessment can be downloaded from the NIC public website at www.odci.gov/nic or obtained from Karen Monaghan, Acting National Intelligence Officer for Economics and Global Issues.
NIC ICA 2003-09
SARS: Down But Still a Threat
August 2003
Scope Note (U)
This Intelligence Community Assessment (ICA) was requested by Secretary of Health and Human Services Tommy Thompson and Ambassador Jack Chow, Deputy Assistant Secretary of State for International Health Affairs.Ā It highlights the evolution of Severe Acute Respiratory Syndrome (SARS) and the potential implications of the disease for the United States under several scenarios; this paper does not attempt to provide a scientific assessment of the epidemiology of SARS.Ā Even though SARS has infected and killed far fewer people than other common infectious diseases such as influenza, malaria, tuberculosis, and HIV/AIDS, it has had a disproportionately large economic and political impact because it spread in areas with broad international commercial links and received intense media attention as a mysterious new illness that seemed able to go anywhere and hit anyone.
As the first infectious disease to emerge as a new cause of human illness in the 21st century, SARS underscores the growing importance of health issues in a globalized world.Ā The December 1999 unclassified National Intelligence Estimate, The Global Infectious Disease Threat and Its Implications for the United States, warned that new and reemerging diseases would pose increasing challenges to the United States and the rest of the world.Ā The 1999 Estimate highlighted several key health trends which track with the emergence of SARS:
The forces of globalization, which are speeding the spread of infectious diseases and amplifying the impact, also are giving us better tools to protect human health.
Major infectious disease threats to the United States and the world, like HIV/AIDS, will continue to emerge, challenging our ability to diagnose, treat, and control them.
Infectious diseases will loom larger in global interstate relations as related embargoes and boycotts to prevent their spread create trade frictions and controversy over culpability.
In addition to coordinating the draft within the Intelligence Community, the National Intelligence Council asked several health experts to review the paper as part of its effort to capitalize on expertise inside and outside the government.Ā The experts included Dr. Anthony Fauci, Director of the National Institute of Allergy and Infectious Diseases at the National Institutes of Health; Dr. Steve Ostroff, Deputy Director, National Center for Infectious Diseases, Centers for Disease Control and Prevention (CDC); and Dr. Joshua Lederberg, Professor Emeritus at Rockefeller University and Nobel Laureate.Ā The NIC also shared the draft with counterparts in Canada at the Privy Council Office, Intelligence Assessment Secretariat.Ā
Key Judgments (U)
The wave of Severe Acute Respiratory Syndrome (SARS) has been overcome, but SARS has not been eradicated.Ā Although the World Health Organization declared on 5 July that all transmission chains of SARS had been broken, many health experts fear it could return again in the fall when cooler temperatures return in temperate areas.Ā We remain vulnerable.
The possible presence of animal reservoirs of the coronavirus that causes SARS and the lack of a reliable diagnostic test or a vaccine preclude eradication.
If a resurgence of SARS this winter coincides with the annual outbreak of influenza, identifying and isolating suspected SARS cases will be much more difficult.Ā SARS also could mutate, altering the symptoms, transmissibility, or lethality of the disease.
As the first line of defense, healthcare systems and workers are particularly vulnerable.Ā Moreover, most wealthy countries have little recent experience implementing large-scale quarantine and isolation programs, and poor countries already have inadequate health surveillance and infection control procedures.
The emergence of SARS illustrates the challenge of battling infectious diseases in an increasingly globalized world.Ā Global links have sped the geographic spread of the disease and amplified the economic and political impact.Ā
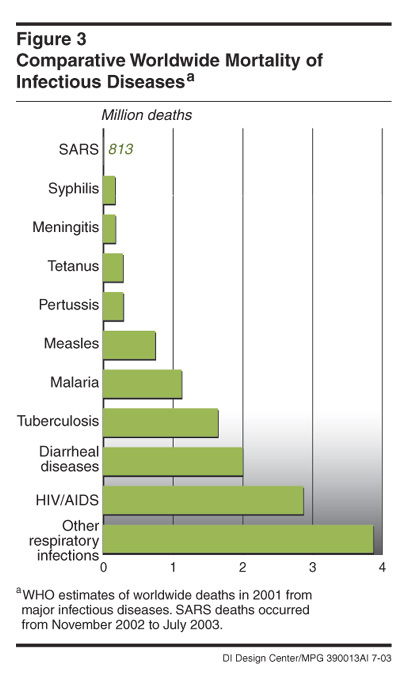
Although SARS has killed far fewer people than die each year from more common maladies such as pneumonia, influenza, malaria, tuberculosis, and HIV/AIDS, it generated significant attention and created a sense of urgency to respond because it was a mysterious new illness that seemed able to go anywhere and hit anyone.
SARS hit parts of Asia and Canada with extensive commercial links to the rest of the world.Ā Although the economic impact, particularly in China, was less severe than initially forecast, SARS wreaked havoc on the tourism and travel industries, erasing revenues and jobs.Ā
The same forces of globalization that drove the spread of SARS also have been key to managing it.Ā Modern advances in communication, science, and travel almost certainly helped alert people more quickly to the disease, facilitated a stronger national and international response, and sped research efforts to help contain the disease.
Political leadership has been a key variable in managing the epidemic.Ā China’s efforts to hide the initial outbreak allowed SARS to build up dangerous momentum before Chinese officials became more open, while Vietnam’s willingness to promptly highlight the threat and seek international assistance helped offset the country’s weak healthcare system.Ā The more SARS spread, the tougher countries became in implementing control measures, including quarantining and isolating people to stop its transmission.
The intense focus on SARS has opened a window of opportunity for the United States and the WHO to pursue longer-term bilateral and multilateral cooperation on health issues.Ā
Three Scenarios
The future course of SARS will depend on a host of complex variables, making forecasting difficult.Ā We constructed three scenarios to highlight various challenges that SARS might pose in the future.Ā Complexity and uncertainty preclude assessing the relative likelihood of any one of the three.SARS Simmers.Ā SARS could resurface this fall but be limited to random outbreaks in a few countries, rendering it more of a public health nuisance than a crisis.Ā Rapid activation of local and international surveillance systems would be key to containing the spread.ĀĀĀ
Political and economic reverberations still would occur, with some companies and investors looking to reduce their exposure in East Asia, particularly China.ĀĀĀ
SARS Gains a Foothold in Poor Countries, Regions.Ā SARS could spread to poor countries in Africa or Asia, potentially generating more infections and deaths than before but with relatively little international economic impact.Ā The risk of spread would continue, however, even if SARS emerged in poor countries or isolated regions of Russia and China with weak healthcare systems.
The World Health Organization and US Centers for Disease Control and Prevention probably would come under intense pressure to provide money and technical assistance to compensate for weak healthcare systems.Ā
Some isolated countries such as North Korea probably would resist outside assistance, even at the risk of putting their own citizens at risk.Ā Some repressive regimes hit by SARS are likely to employ brutal tactics to quarantine and isolate people, possibly sowing division among outside countries and multilateral organizations over how to respond to apparent human rights violations.
SARS Resurges.Ā SARS could come back this fall in the places it hit before—such as China, Taiwan, Canada, and Singapore—or hit harder in other well-connected places like the United States, Japan, Europe, India, or Brazil.Ā Even if the number of infected persons were not significantly greater, the resurgence of the disease in globally linked countries probably would generate a significant impact again.Ā
The return of SARS to Asia is likely to cause somewhat less disruption the second time as citizens learn to live with the disease, but more multinational companies probably would reduce their exposure in the region if they concluded that SARS posed a long-term health challenge.Ā
Bigger outbreaks in Europe or the United States would hit a whole new set of business and government players, potentially doing serious damage to trade and growth.Ā
Discussion
The Global Health ChallengeĀ
The emergence of Severe Acute Respiratory Syndrome (SARS) illustrates the challenge of battling infectious diseases in an increasingly globalized world.Ā SARS is the latest of more than 35 new or reemerged infectious diseases over the last 30 years.Ā Infectious diseases have long raged through human communities, but forces of globalization—including rapid growth in international trade and travel and increasing urbanization—have amplified their spread and impact.Ā These same forces of globalization, however, also have led to significant advances in communication, travel, and technology, which have aided in the fight against infectious diseases.
On balance, infectious disease pathogens have the upper hand because they constantly evolve new mechanisms that can exploit weak links in human defenses.
SARS has subsided for now, but many health experts warn that it is likely to come back when cooler weather returns to temperate areas, bringing a resurgence of respiratory infections.
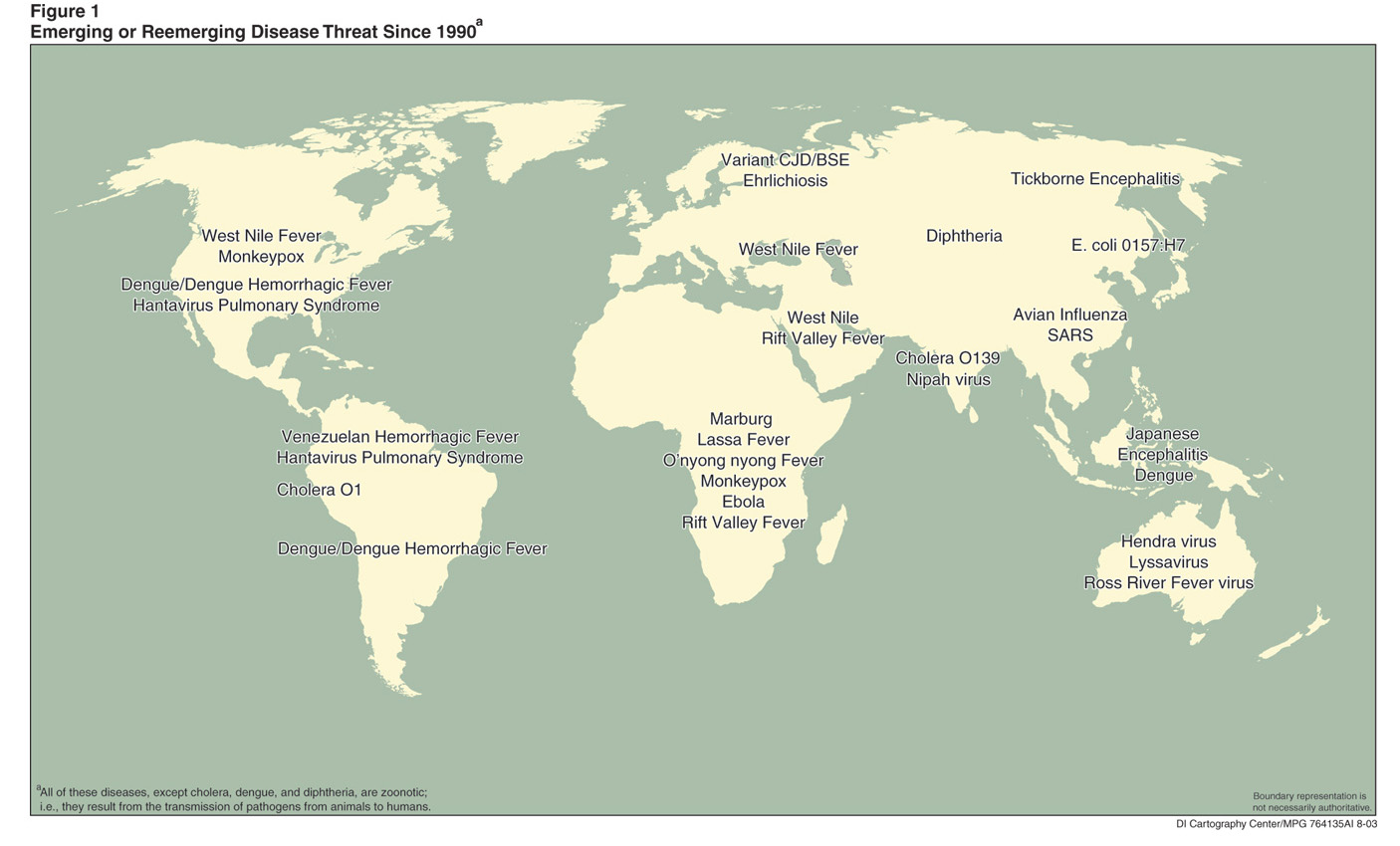
Downsides of Globalization.Ā Population growth and development are bringing more people into contact with non-domesticated animals, introducing new diseases more frequently into the human population.Ā The transmission of pathogens from animals to humans is a process called zoonosisĀ (see map).Ā Some researchers believe that SARS may have originated in China in animals such as wildcat species that were trapped and sold as food in exotic markets.Ā In mid August 2003, China lifted the ban on the sale and consumption of exotic animals imposed during the SARS epidemic.
HIV/AIDS, monkeypox, and hantavirus are other infectious diseases believed to have originated in animals.
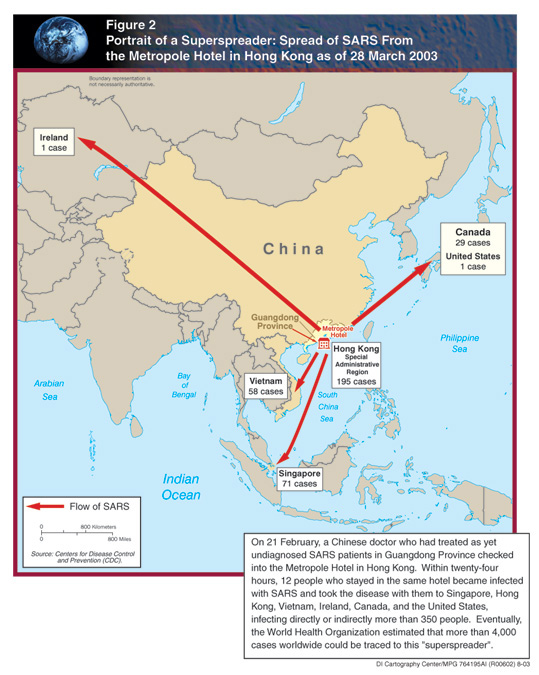
Modern travel and labor migration patterns played a key role in spreading SARS after it emerged in November 2002 in Guangdong Province, China.Ā From Guangdong, the disease made its way to Hong Kong and then to Vietnam, Singapore, and Taiwan as well as Europe and North America.
Within China, as many as 180 million people are considered migrant labor, moving between rural areas, cities, and manufacturing centers in search of employment.
Asia has become a major hub for business and tourist travel, putting millions of passengers within 24 hours of almost every major city in the world, providing little time to identify and isolate people infected with diseases that may take several days to show symptoms.Ā
More people also are migrating overseas to find jobs, and travel by workers and their families can spread diseases.Ā For example, a Filipino nurse working in Toronto contracted SARS and transmitted it to family members on a visit to the Philippines.
In addition to spreading the disease geographically, global links also have amplified the economic and political impact of the disease.Ā Even though SARS has killed far fewer people up to now—around 815—than those who die each year from more common maladies such as pneumonia, influenza, malaria, and tuberculosis, as a new disease it was more disruptive and generated more attention.Ā The disease exhibited some characteristics of a potentially explosive epidemic in the early stages, and SARS hit countries that have extensive commercial links with other parts of the world, generating widespread economic disruptions and media attention.
The outbreak of SARS in Asia and Canada disrupted a wide-ranging global network of businesses increasingly dependent on international trade and travel.Ā Airlines were the highest profile economic victims, but service industries like tourism and supply chains in industries as diverse as seafood and microchips also were affected.
Intense media attention and uncertainty about the disease fueled widespread fear, even in some areas without any cases, exacerbating economic disruptions.
The suspicion of Asians as carriers of the disease reduced patronage of Asian businesses and communities in the United States and sparked travel bans against Asian tourist groups and conference participants worldwide.
Benefits of Globalization.Ā Intense international media coverage facilitated by global communication networks increased pressure on governments to respond effectively to SARS and prompted many citizens and healthcare workers to be vigilant in taking precautions, monitoring symptoms, and seeking early treatment.
China initially tried to cover up SARS as it did with other diseases in the past, but international media scrutiny and leaks to the press led Beijing to publicly acknowledge and respond to the disease.
The public has been able to track the evolution of the disease more closely with everything from text messaging on cell phones to publicly and privately run websites; Singaporeans could even watch a special public service television channel devoted to SARS.
Modern communications and medical technologies provided key tools to combat SARS.
Health workers utilized the World Health Organization’s (WHO) global network of research facilities to share data and speed the identification of the virus causing SARS.
International medical journals took the rare step of promptly publishing research on SARS on the Internet prior to hard copy publication.
Thermal imaging equipment was acquired in numerous countries in an effort to screen large numbers of people for high fevers.Ā Hong Kong employed software to track the spread of the disease in urban areas, and some countries employed cameras and electronic bracelets to help security officials enforce home quarantines.
Economic and Political Fallout of SARS
Government and private sector economists have had difficulty calculating the costs of the SARS epidemic.Ā Early on, forecasters estimated that the macroeconomic impact would be negligible but hastily cut growth estimates for several economies, including China, as the disease spread, cases mounted, and the situation appeared to be out of control.Ā Service industries, particularly airlines and tourism, were affected immediately.Ā SARS began to threaten the retail and manufacturing sectors, particularly in China, when business trips and trade fairs were canceled, new orders were placed on hold, and investors delayed new expansion and constructions plans.Ā
In late April, the World Bank cut its growth forecast for East Asia to 5.0 percent—from 5.8 percent in 2002—due in part to SARS.
In early May, the Asian Development Bank warned that East Asia could lose $US 28 billion in income and output if the disease continued until September.Ā
Several investment banks shaved up to one percentage point off China’s growth forecasts and cautioned that a more serious slowdown could occur if SARS were not brought under control by July.
North Korea imposed tight border restrictions and quarantines, slowing trade flows and temporarily closing a lucrative new tourist resort.
Recent data suggest that growth in most countries plummeted in April and May but started to recover as the disease was brought under control, reports of new cases dwindled, and the WHO removed countries from its travel advisory list.Ā Most notably, no major disruptions in trade and investment flows occurred.Ā Moreover, most factories in China, including those in Guangdong where the disease originated, continued to operate even during the height of the epidemic.Ā In some countries, monetary and fiscal stimulus packages also helped to cushion the blow.Ā
Certain locales, notably Hong Kong, Beijing, and Toronto, were hurt more than others.Ā Moreover, additional indirect costs—the so- called “SARS tax”—probably will be incurred by businesses consumers, governments, and nongovernment agencies.Ā
Collectively, the ASEAN countries—Brunei, Cambodia, Indonesia, Laos, Malaysia, Myanmar, the Philippines, Singapore, Thailand and Vietnam—are estimated to have lost $US 25 billion to $US 30 billion, mostly in the tourism, service, aviation, and restaurant sectors.
Although China is forecast to achieve growth of 7 to 8 percent this year, the economies of China and Hong Kong will take longer to recover because the tourism, transport, communication, food, and entertainment industries suffered substantial losses.
Most analysts forecast that SARS would shave a minimal amount off Canada’s 2003 growth but cut 1 percent off Toronto’s $200 billion economy.Ā
SARS dealt a body blow to the travel and tourism industries, already facing a slowdown from post-9/11 terrorism concerns.Ā They will be slow to recover.Ā Business travel has resumed more rapidly as firms catch up on a backlog of deals, but tourist travel is far below last year’s levels.Ā Hotels in Asia are cutting room rates in a bid to attract customers.Ā
An industry trade group estimates the tourist sector in China, Hong Kong, Singapore, and Vietnam will lose up to $US 10 billion and 3 million jobs this year because of SARS.Ā
Airlines have restored most canceled flights, but carriers will have difficulty recouping lost revenues, and some may be forced into bankruptcy.Ā The airline industry’s slow recovery will be a further drag on the aviation industry.Ā Asian airlines were to account for one-quarter of Airbus deliveries and 30 percent of Boeing’s deliveries in 2003.Ā Several Asia-Pacific carriers asked Airbus and Boeing to postpone deliveries of new aircraft.Ā Both manufacturers have been counting on robust growth in the Asian travel market to boost revenues.
Anecdotal evidence suggests that some export-oriented industries, particularly clothing manufacturers, temporarily shifted some orders to Bangladesh, Turkey, India, and Pakistan.Ā Foreign electronics manufacturers, including a large Japanese electronics firm, shifted some production to plants in Philippines and Malaysia with highly specialized sectors and relatively low costs. There is no evidence to suggest that foreign manufacturers pulled out investments or permanently shifted production outside China or East Asian production plants.Ā Some multinationals probably have begun to rethink the costs and benefits of concentrating investment in one country or region, however.Ā
Over the last decade, China has attracted massive amounts of foreign direct investment (FDI)—$53 billion in 2002—thanks to its reputation as a low-cost and relatively low-risk manufacturing locale with a rapidly growing domestic market.Ā
SARS has had minimal impact on global semiconductor production, even though nearly 80 percent of production in this $US 8 billion industry is located in Asia, largely in Taiwan and China.
None of the semiconductor operations was forced to curtail production, although SARS disrupted some visits by foreign equipment suppliers and prompted the temporary closing of some Hong Kong sales and marketing offices.Ā
Table 1:Ā Economic Impact of SARS
The chart below reflects estimates for 2003 based on second-quarter data, but the delayed impact and potential for recurrence in the fall suggest that it may be premature to measure the full impact on growth.
Economy
GDP
Employment
Sectoral Impact
Stimulus Packages
Cumulative SARS cases (deaths)*
China
Early predictions of severe impact revised, forecasts suggest strong growth of 7 to 8 percent for 2003.Ā
Major impact on jobless rate, especially among migrant workforce; unemployment nearly doubles to over 8 million.
Retail sales and restaurant sector stall, particularly in urban areas.Ā Export and manufacturing have proven more resilient.Ā
No comprehensive package, but some ad hoc measures for service sector, including temporary tax cuts.
5327 (348)
Hong Kong
Official growth estimate cut to 1.5 percent from earlier forecasts of 3 percent.
Unemployment hits record high 8.3 percent over March-to-May period, could swell to 10 percent by yearend.
Tourism and retail sector ravaged, but few signs SARS has hurt trade.Ā Air traffic fell 80 percent in May.
A US $1.8 billion relief package, including rent reductions and tax rebates, especially for hardest hit businesses.
1755Ā (298)
Taiwan
Official growth estimate cut to 2.7 percent from earlier forecasts of 3.7 percent.
Minimal impact as employers cut pay and grant unpaid leave but miss target of reducing unemployment to 4.5 percent in 2003.
Tourism and retail sectors hardest hit.
Emergency relief and economic stimulus packages worth $3.7 billion, and a three-year $8.6 billion public works program.
671Ā (84)
Singapore
Private sector growth forecasts cut to 1 percent from earlier estimates of more than 2 percent.
Unemployment expected to rise to record high 5.5 percent; wage freezes and cuts implemented.
Hospitality and travel industries most affected; also hit retail stores and restaurants.
US $130 million relief package targeted at SARS-affected sectors.
206Ā (32)
Thailand
Private sector forecasts put growth as low as 4.2 percent, down one percentage point from 2002.
First quarter employment data show no impact.
Tourist arrivals were down 10 percent in the first five months this year; exports also suffered.
None implemented.
9 (2)
Canada
Growth expected to slow to 2.2 percent, down one percentage point from earlier forecasts due to SARS, mad-cow, other problems.
Unemployment increased in May to 7.8 percent; thousands of jobs lost in the hospitality sector nationwide.
Lost tourism and airport revenues amounted to $950 million, $570 million in Toronto alone.
In July, the Bank of Canada cut interest rate one-quarter to 3 percent.
250Ā (38)
* Information from WHO as of July 8, 2003.Ā Political Impact.Ā SARS seriously tested the leadership skills of politicians and civil servants in every country affected.Ā The public was quick to criticize leaders in China, Canada, Hong Kong, and Taiwan for failing to grasp the seriousness of the situation, to act quickly to contain the spread, and to accept responsibility for missteps.Ā In some countries, public confidence in the ability of government leaders and state institutions to protect them may be permanently damaged.Ā
In China, SARS intensified behind-the-scenes jockeying between President Hu Jintao and his predecessor, Jiang Zemin, who initially downplayed the disease. ĀHu publicly acknowledged the threat of SARS, allowed greater media coverage of the crisis, and sacked one of Jiang’s loyalists as Minister of Health.
In Canada the Prime Minister, Premier of Ontario, and Mayor of Toronto drew fire from media and opposition party critics accusing them of failing to respond effectively and address public fears.
In contrast, the WHO and Centers for Disease Control and Prevention (CDC) lauded the Vietnamese government’s swift action and willingness to accept outside assistance, noting these factors were key to its success in containing the spread of SARS.Ā In Singapore, the public expressed confidence and support for the government’s rigorous efforts to identify and isolate suspected SARS patients.Ā An early April poll showed three out of four Singaporeans were confident that the government could stop SARS.Ā
Tracking the Downturn in SARS
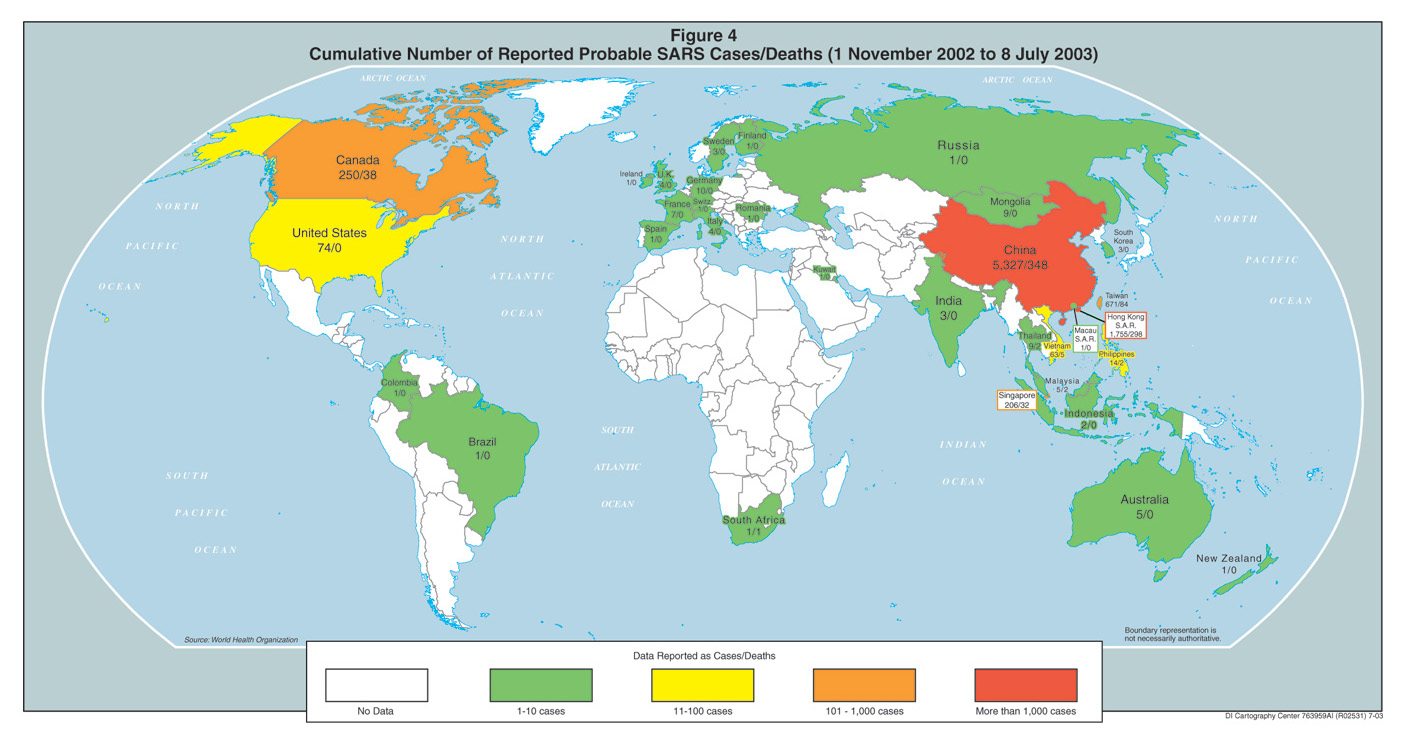
Since WHO first issued a global alert about SARS in March 2003, almost 8,500 probable cases have been reported from 29 countries around the world, with most cases (over 7,000) occurring in China.Ā At one point in May, over 180 new infections were being reported daily, mostly in China.
The number of SARS cases peaked in May and steadily declined worldwide with the WHO declaring on 5 July that all transmission chains of the disease had been broken.Ā The decline may reflect a seasonal retreat of the disease in warmer months, which is common for respiratory illnesses in temperate climates.Ā Nonetheless, the downturn clearly illustrates that, even in a globalized world, the old-fashioned work of identifying and isolating suspected cases, tracing and quarantining others who might be exposed, and issuing travel advisories can control an emerging disease.
Most countries hit by SARS had not used traditional public health tools such as quarantine and isolation on such a large scale for decades, which slowed the containment.
Governments also had to mobilize enormous resources to implement large-scale quarantine operations.
Surveillance.Ā The first line of defense in arresting the spread of SARS has been the success in identifying possible cases—despite the lack of a proven screening test and symptoms common to many respiratory ailments.Ā Taking people’s temperature generally has been the simplest, most cost-effective means of initial screening for possible SARS cases, followed by clinical examination for respiratory symptoms in those with fevers.1
Singapore issued over a million SARS toolkits with thermometers and facemasks to every residence in the country.Ā Residents were regularly stopped at office buildings, schools, and other public places for temperature checks.
China mobilized local party and government officials, including 85 million family planning workers, to try to monitor citizens for symptoms.Ā China also mobilized its large militia to provide the rural public with instructions on SARS prevention.Ā The government distributed tens of thousands of thermometers to the provinces.
- After WHO confirmed that SARS could be transmitted on airline flights, including 22 infections traced to a single flight in March, airlines have become more stringent at keeping people who might be infected off airplanes.
SARS Basics
Origins.Ā The SARS epidemic spread rapidly because people had little immunity to the newly emerged coronavirus that causes the disease.Ā Close contact with sick individuals appears to be the primary means of virus transmission, although research indicates that SARS does not transmit as easily from person-to-person as more common diseases like the cold or flu.Ā The disease spread most rapidly among healthcare workers and family members of infected individuals.Ā Evidence indicates that the virus also is spread through contact with inanimate objects contaminated with virus-containing secretions. ĀRecent detection of a related coronavirus in wildcat species in China raises concerns that SARS may continue to have an animal reservoir, which would complicate control efforts.
Symptoms.Ā SARS can progress rapidly from fever and cough to serious pneumonia after an average four-to-six-day incubation period, with up to 20 percent of patients needing mechanical ventilation to survive.Ā In some patients, progression to pneumonia may be delayed.Ā Death may occur several weeks to months after initial symptoms.
Diagnosis.Ā Accurate, rapid screening diagnostic tests for SARS are being developed but are not yet licensed in the United States.Ā During the epidemic healthcare workers generally relied on clinical symptoms for detection.Ā WHO defines a suspected SARS case as someone with a temperature over 38 degrees Celsius, a cough or difficulty breathing, and one or more of the following exposures:Ā close contact with a person who is a suspect or probable SARS case, or someone who has lived in or visited a region with SARS transmissions.Ā A “probable case” is a suspected case with radiographic evidence of pneumonia or positive laboratory tests that may take days to weeks to complete.
Treatment.Ā No proven therapy is available for severe SARS pneumonia cases.Ā Most clinicians employ respiratory support, antibiotics, fever reduction, and hydration.Ā Some Chinese doctors have used steroids and the antiviral drug ribavirin with varying degrees of success.
Fatalities.Ā Although the overall lethality of SARS is higher than initially believed, most deaths continue to be among older patients and those with underlying health problems, such as diabetes or hepatitis B.Ā The WHO reported in May 2003 that death rates vary substantially by age:
Less than 1 percent in persons 24 years or younger.
Up to 6 percent in persons 25 to 44 years old.ĀĀĀĀĀĀ
Up to 15 percent in persons 44 to 64 years old.
Greater than 55 percent in persons aged 65 or older.
Preliminary reports on nonfatal cases showed SARS patients required longer hospital stays—an average of three weeks for those under 60 years of age—than patients with other typical respiratory viruses, raising the economic costs of the SARS outbreak.Ā Moreover, preliminary evidence suggests that some people who survive SARS could suffer long-term respiratory damage that increases health complications and costs.Ā
The World Health Organization:Ā Playing Fairly Well with a Weak HandĀ
The World Health Organization (WHO) issued an international health warning on SARS in March 2003 and travel advisories regarding particular regions hit by the disease.Ā The WHO, in collaboration with the US Centers for Disease Control and Prevention (CDC) and other organizations, worked to identify the cause of the disease, assisted local investigators, and provided guidance on control measures.
The SARS experience highlights the bureaucratic and technical limitations WHO faces in trying to identify and control the international spread of infectious diseases.Ā Under existing international health regulations, countries are only required to report to WHO outbreaks of yellow fever, cholera, and plague.Ā With these diseases, WHO, the United Nations, and domestic officials have the authority to intervene and prevent the movement of people and goods to avert cross-border transmission.Ā With other diseases, WHO plays an advisory role, including issuing travel advisories and offering advice to member governments on screening procedures.Ā Unless a country invites in WHO investigators, WHO has a limited ability to respond to outbreaks.Ā Moreover, WHO has limited capability to investigate suspicious outbreaks before a country officially reports them.
The World Health Assembly, the body that oversees the WHO, recommended expanding the list of reportable diseases by 2005 to include notification for public health emergencies of international concern.
In 2000, WHO, with assistance from the Canadian Government, set up the Global Outbreak Alert and Response Network to enhance global surveillance, detection, and response to emerging infectious diseases.Ā It uses an electronic collection system to scan worldwide news reports, websites, discussion groups, and other open source information networks for rumors or reports of disease outbreaks.Ā These notifications trigger WHO staff to notify country representatives, who query national authorities for more information about possible disease outbreaks, bypassing official government notification channels.
Despite these advances, the system may not have picked up early clues to the SARS outbreak.Ā The electronic monitoring system currently only searches in English and French, although WHO plans to add search capabilities in Arabic, Chinese, Russian, and Spanish.Ā In addition, once WHO receives notification, country cooperation is essential to validate the outbreak, something Chinese officials avoided until late in the outbreak.
Even though checks of passengers at airports were relatively effective at keeping infected people off airplanes, some lapses did occur.Ā
Japan installed infrared thermometers to monitor passengers at Tokyo’s international airport after voluntary testing proved ineffective, but press reports indicate that the machines cannot keep up with all travelers at peak times.Ā
An Asian man suspected of having SARS boarded a flight to the United States in May because his flight left before lab results were received and he had no other symptoms.Ā
Quarantines and Isolation.2Ā As SARS spread and political and economic stakes rose, countries took tougher measures to contain it.Ā Some countries resorted to strong steps, such as closing schools despite the low number of cases among children, probably to compensate for weaknesses in their health-care infrastructure.Ā Open societies seemed to have trouble enforcing quarantine orders.Ā
Some Chinese citizens fled cities and industrial hubs in response to early government efforts to isolate suspected cases and quarantine their contacts.Ā Subsequently, Beijing forcibly locked both patients and healthcare workers in hospitals during the peak of infections, and the government instituted fines for people violating isolation orders and employed citizens to keep outsiders out of various villages.Ā Shanghai officials announced in late May they had quarantined nearly 29,000 people in the previous two months.
Canada threatened those who violated quarantines with fines or court-ordered isolation after some people defied voluntary measures, but news reports indicate that some people violated quarantines when the SARS threat appeared to be fading.
Singapore’s strict quarantines proved particularly effective in bringing the disease under control.
Sometimes the most effective isolation and quarantine policies raised concerns about political freedom and human rights.Ā For example, India and Thailand at one point isolated foreign visitors from countries that had SARS outbreaks, even though they did not have symptoms or known exposures.
North Korea, which has quarantined entire areas to deal with epidemics in the past, imposed such tight restrictions for SARS that it constrained some international aid flows.
The World’s Quick Response to SARS
Several factors appeared to facilitate a faster international reaction to SARS in comparison to other diseases in recent decades.
Fear and Uncertainty.Ā The rapid geographic spread of the mysterious illness created a sense of urgency to respond to a disease that seemed able to “go anywhere and hit anyone.”
Stronger Leadership.Ā The World Health Organization took a more public, activist stance in sounding the alarm and mobilizing the global response.
Scientific Advances.Ā New tools and techniques allowed researchers better and faster ways to study everything from patterns of lung damage to the genetic sequence of the coronavirus.
Heightened Awareness of BW Threat.Ā Concerns about the threat posed by biological weapons enhanced the ability and speed of many countries to identify new infectious diseases.
Concern About Missing “Another” AIDS.Ā Some health officials acknowledge they reacted more quickly to SARS partly due to fears that the world’s slow response in the 1980s to the emergence of HIV/AIDS allowed the disease to build up devastating momentum.
Political Leadership.Ā A key variable in managing the SARS epidemic was the willingness of political leaders to raise public awareness of the disease, focus resources, and speed the government response.Ā As noted above, Vietnamese leaders promptly acknowledged the SARS threat at an early stage in the outbreak and sought international help.Ā In contrast, China’s political leaders clearly exacerbated the situation by initially suppressing news of the disease.
Reasons to Stay on Guard
Despite the downturn in cases, SARS has not been eradicated and remains a significant potential threat.Ā Senior WHO officials and many other noted medical experts believe it highly likely that SARS will return.Ā SARS, like other respiratory diseases such as influenza, may have subsided in the northern hemisphere as summer temperatures rise, only to come back in the fall.ĀĀ
Most infectious diseases follow a similar epidemiological curve, emerging, peaking, and declining over time to a steady state, but the number of infections, the lethality, and length of time can vary enormously.
Even as WHO officials removed the last of its travel advisories for SARS early this summer, officers repeatedly emphasized the risk that the disease would be back.
Some experts caution that SARS might even lay low for several years before reappearing, as diseases such as Ebola and Marburg have done.ĀĀ
The apparent reservoir of the coronavirus in animals, Bejing’s decision to lift the ban on sales of exotic animals, and lack of a reliable diagnostic kit, vaccine, or antiviral drug are factors that preclude eradication.Ā
No Reliable Screening Tests.Ā Diagnosis remains almost as much an art as a science as long as no proven screening test has been developed.Ā Diagnostic kits currently under development can catch only about 70 percent of SARS cases, and their utility for widespread deployment is not yet known.Ā SARS is difficult to detect, particularly in the early stages, even for countries with the most modern medical capabilities, raising the risk that healthcare workers will miss mild cases.Ā Moreover, there is little prospect of a vaccine in the short-term.Ā
Various countries have different definitions of suspected and probable cases and have changed the definitions over time.
SARS Could Mutate.Ā Natural mutations in the coronavirus which causes SARS could alter basic characteristics of the disease, but whether a mutation would make SARS more or less dangerous is impossible to predict.Ā A significant increase in the transmissibility or lethality of SARS obviously would pose greater health risks and raise fears around the globe.
Mutations could be particularly problematic if they alter the symptoms associated with SARS, making it harder to identify suspected cases.
Researchers are studying a group of Canadians who tested positive for the SARS virus last spring but never got sick in order to see if they still might have infected others.
Mutations also would complicate the development of a treatment or vaccine, which already probably is several years away.
Difficult to Maintain Vigilance.Ā The willingness of healthcare workers to serve in the face of significant infection risks has been a key variable in the battle against SARS and other emerging diseases.Ā Most healthcare workers in countries hit by SARS toiled long hours under dangerous conditions.Ā The rate of infection among hospital workers was much higher than among the general public, underscoring the difficulty even professionals had in maintaining stringent infection control procedures.
At one point 20 percent of those infected in Hong Kong were nurses, and over 300 healthcare workers were infected within a 17-day period in China during April.
Some health workers refused to work in SARS wards.Ā This problem is likely to grow in both rich and poor countries if the disease resurges.
In Taiwan, where over 90 percent of SARS infections occurred in hospitals, over 160 health workers quit or refused to work on SARS wards.Ā The government threatened to revoke their professional licenses.Ā
The Chinese government fired at least six doctors who refused to treat SARS patients and barred them from practicing for life.Ā China also tried to encourage healthcare workers by launching public relations campaigns hailing the work of the Angels in White, and Beijing offered bonus pay and staffed SARS hospitals with Army medical staff.Ā
Press reports in Canada indicate that some nurses refused to work in SARS wards in Toronto despite a doubling of their wages and lobbied for an official government inquiry on the handling of the epidemic.
Shortages in trained healthcare personnel were exacerbated when many healthcare workers fell ill to SARS and were replaced by workers with less training.
Taiwan appeared so eager to declare victory over SARS that it relaxed its standards before the disease was brought under control.Ā Press reports suggest that some healthcare workers were so fatigued from the crisis that they cut corners.
Canadian officials acknowledge that the second outbreak in Toronto resulted from hospitals relaxing infection control regimes too quickly.
SARS Scenarios
Faced with these uncertainties, we have constructed three scenarios to consider potential trajectories for the disease and the implications for the United States.Ā We have not attempted to identify a most likely scenario because the future course of SARS will depend on a host of complex variables, including the scope of present infections, mutations in the virus, the vulnerability of host populations, how individuals and governments respond, and chance.Ā
Scenario One:Ā SARS Simmers
SARS could resurface this fall but be limited to random outbreaks in a few countries.Ā Rapid activation of local and international surveillance systems and isolation procedures would be key to identifying suspect cases and containing the spread.Ā Initially, some cases might elude detection by hospital workers and airport personnel, who have relaxed screening procedures since the disease ebbed.Ā Smaller, poorly-funded transit facilities would remain vulnerable because they lacked trained staff and equipment to effectively monitor all passengers.Ā
In most affected countries, the small number of cases and transmission would render SARS more of a public health nuisance than a crisis.
Some countries would be tempted to hide a resurgence.Ā China’s experience demonstrated that hiding an outbreak is increasingly difficult and costly in a globalized world, but some governments still probably calculate that transparency also has drawbacks.Ā Indeed, the economic repercussions of WHO travel advisories for SARS probably reinforce the incentives countries have to hide or underreport cases.
The WHO had to lean on Beijing throughout the crisis to share data.
Some countries over the past decade have not acknowledged HIV/AIDS cases in the military for security reasons, suggesting they would withhold information on other diseases that might affect readiness.
Even if new SARS outbreaks were sporadic and small-scale, economic, political, and psychological ripples would occur.Ā China faces the biggest risks.Ā Although foreign investors are unlikely to withdraw substantial amounts of FDI, firms with considerable exposure to China might redirect a percentage of new investment to other locations to diversify their manufacturing operations.Ā Companies that already have temporarily shifted some production outside China probably would establish more permanent arrangements.Ā
Companies and governments outside China probably would attempt to exploit these concerns by more aggressively trying to turn temporary production into longer-term investments.
Multinationals also are likely to become more concerned about the “SARS tax” on their businesses, including increased healthcare expenditures for expatriate employees and expanded insurance to cover the risk to operations and personnel from infectious diseases.Ā Some firms probably would calculate that the risks of frequent business travel outweighed the costs and switch to teleconferencing, telecommuting, and
e-commerce.Ā
SARS has alerted companies to the potential operational disruptions caused by a contagious disease, risks that are rarely priced into business costs or considered in contingency planning.Ā
Whereas previous business continuity plans focused on data protection and recovery, businesses probably will begin to consider plans that involve protection of human resources, backup teams, and alternate locations for operation.
Paradoxically, keeping SARS out of the United States might become more difficult as fewer cases are seen, because health, transportation, and security workers are more likely to drop their guard in monitoring for infected people if only a few cases pop up now and then.Ā
The US status as a major hub for international travel increases the statistical risk that lapses in surveillance abroad could facilitate the spread of SARS to American cities.
It is difficult for many visitors to acquire visas for travel to the United States; thus they probably would be inclined to withhold information that could complicate their visit.
Scenario Two:Ā SARS Spreads to Poor Countries, Regions
SARS could gain a foothold in one or more poor countries, potentially generating more infections and deaths than before but with relatively little international economic impact.Ā Few poor countries have had SARS appear on their doorstep up to now because most have relatively few links to the affected regions, but the longer the disease persists the more likely it is that SARS will spread more widely.
Impoverished areas of Africa, Asia, and Latin America remain at potential risk for SARS because of weak healthcare systems and vulnerable populations.Ā Even a small number of cases in large, under-developed cities such as Dhaka, Kinshasa, or Lagos could generate a large number of victims in a short period.
No evidence thus far suggests that people with malaria or HIV/AIDS are more susceptible to becoming infected by SARS, but experience indicates that diseases are more lethal among sick and malnourished populations.Ā Sub-Saharan Africa has the highest concentration of HIV-infected people in the world, and those with full-blown AIDS have severely deficient immune response.
Most poor countries would have trouble organizing control measures against SARS, especially if the disease gained momentum before it was identified by healthcare workers.Ā Most countries have inadequate hospital facilities to effectively isolate large numbers of patients, and most hospitals even lack the resources to provide food and care to patients.
Voluntary home quarantine might not be viable in crowded urban slums, where large families might share small dwellings and people might have to go out each day for food or work.
Identifying and tracking down people who might have been exposed probably would be substantially more difficult in countries with poor infrastructure and underfunded local security services.
Repressive countries, fearful that the disease could spark political upheaval, probably would quarantine entire towns or villages with military force or incarcerate quarantine violators.Ā Outside countries and international organizations providing assistance are likely to split over how much to condemn or withhold aid over apparent human rights violations.Ā
The spread of SARS into various poor countries is likely to significantly disrupt local economies while having relatively little impact on broader international markets.Ā
The local impact could be worse than in places like Taiwan and Canada, because people in poor countries are living closer to the margin and governments have less resources for emergencies.Ā In countries with a much smaller pool of skilled workers, the loss of key personnel can have a relatively large effect on society—as HIV/AIDS has illustrated in Africa.
Even poor countries like Bangladesh have at least some global trade and business links that could be disrupted if they were hit by SARS, but the more isolated the country, the smaller the global economic impact probably would be.
The spread of SARS to poor countries also would complicate international efforts to control the disease.Ā
Diagnosing SARS is likely to be more difficult among populations with many preexisting health problems.
Even if SARS claimed hundreds of victims in poor countries, their governments probably would not be inclined to devote substantial resources to the fight when other diseases—such as malaria, tuberculosis, and HIV/AIDS—were claiming many more lives.
The spread of SARS to countries with weak healthcare systems and vulnerable populations also is likely to make the disease appear more transmissible and lethal, heightening public fears in other parts of the world.
Poor, isolated regions of Russia and China would have trouble containing an outbreak, although their governments probably could mobilize more resources to respond once infections began to climb.
Even if SARS outbreaks were limited to poor countries, the persistence of the disease probably would fuel some unease around the world about a broader resurgence.Ā The impact probably would marginally decrease demand for travel and increase demand for medical products.
An outbreak of SARS in poor countries would pose particular challenges for the United States and other governments and multilateral organizations providing assistance.Ā WHO and CDC probably would come under pressure to provide money and technical assistance to compensate for weak healthcare systems.Ā The higher the number of infected people, the more the international community would be called on to do something.Ā
Neighboring countries are likely to press for help with disease monitoring to prevent SARS from spreading into their countries, especially if panic began generating refugee flows.
Repressive regimes like North Korea might accept material assistance but block outside experts from visiting, even at the risk of putting more of their own citizens at risk.Ā North Korea in previous years has been accused of diverting NGO assistance to the military and not allowing outsiders to monitor how it is used.
Scenario Three:Ā SARS Resurges in Major Trade Centers
SARS could stage a comeback this fall in the main places it hit before—such as China, Hong Kong, Taiwan, and Canada—or gain a foothold in other places with extensive international travel and trade links like the United States, Japan, Europe, India, or Brazil.Ā
An outbreak almost certainly would spark another wave of WHO health warnings and travel advisories; Japan already has cancelled an international conference on HIV/AIDS planned for this winter due to fears it would coincide with a resurgence of SARS.
Even if the number of infected persons were not greater in a second wave, an outbreak of SARS in major trade centers again would be likely to have significant economic and political implications.Ā The resurgence of SARS in Asia probably would cause less disruption as citizens, companies, and governments learn to live with it, as they do with other diseases, unless the transmissibility or lethality rose substantially.Ā Nonetheless, a second wave of SARS in Asia probably would prompt some multinationals to modestly reduce their exposure to the region if they concluded that SARS posed a long-term health challenge.
Given the size of the Asian market and low wage-rates, few companies are likely to yank existing production out of China unless SARS debilitates or kills large numbers of workers.Ā Firms probably would divert some future investments to other regions to diversify their supply chains.
Disruptions due to SARS are likely to persuade some companies to loosen just-in-time production chains by creating some cushion in key inventories, increasing costs but not productivity.Ā
Global trade and investment flows could seize up if quarantines shut down factories and shipments.Ā
A substantial decline in China’s manu-facturing sector would reverberate in Southeast Asian economies that provide critical manufactured inputs, raw materials, and energy and disrupts production chains throughout East Asia.Ā
Bigger outbreaks in places such as Europe and the United States would affect new sets of business and government players.Ā The level of public fear almost certainly would be higher in places that had not been affected by the first wave of SARS, driving up social disruption and economic costs.Ā
The economic cost of SARS probably would skyrocket if fears grew about the transmission of the disease in planes or on objects.
Some buyers this spring demanded that Asian manufacturers irradiate their export goods after research indicated that SARS could survive for several days on inanimate objects.
Even the health systems of rich countries could be overwhelmed if the resurgence of SARS cases coincided with the annual influenza epidemic this winter.Ā As long as no quick and reliable test to diagnose SARS exists, people with fevers and a cough could overwhelm hospitals and clinics as healthcare workers struggled to distinguish patients with SARS and isolate them from others.Ā
A pneumonia-like illness erupted in western Canada in mid-August, raising questions among health experts about whether a milder version of SARS had returned.
Surges of people seeking medical care almost certainly would increase the odds of healthcare workers missing some cases.
Some SARS patients have not displayed classic respiratory symptoms, suggesting some “silent” spreaders may not even know they have the disease, and some travelers with mild symptoms might lie about contact with infected persons to avoid quarantine.
Given the high economic and political stakes already seen in the SARS epidemic, some jurisdictions probably would try to fudge health data in an effort to avoid official health warnings or get them lifted more quickly.
Some governments might narrow the definition of “probable” SARS cases to reduce crowding in hospitals, yet such moves could spark tensions with WHO and other countries over the accuracy of data.
Building Better Defenses Against Disease
The emergence of SARS has sparked widespread calls for greater international surveillance and cooperation against such diseases.Ā SARS has demonstrated to even skeptical government leaders that health matters in profound social, economic, and political ways.
The experience with SARS probably will help countries prepare for future disease outbreaks.
Influenza:Ā Lurking Killer
Influenza is an ideal virus for worldwide spread (a pandemic) and many epidemilogists argue that the world is “overdue” for a major influenza pandemic.Ā When a new type of flu virus emerges from a reassortment of animal and human viruses to which humans have no prior immunity, a pandemic may ensue.Ā Scientists believe the past two influenza pandemics originated in China where people live in close contact with birds and swine, the major sources of animal flu viruses.Ā Influenza spreads even more quickly than SARS because flu can be transmitted efficiently through the air.Ā As a result, close contact is not required for people to become infected, making it almost impossible to trace and isolate ill people who are spreading the disease.
Three major flu epidemics stand out in modern US history:
1918-19:Ā “Spanish Flu” caused 20-50 million deaths worldwide, including 500,000 in the United States.
1957-58:Ā “Asian Flu” originated in China and spread globally, killing around 70,000 Americans.
l968-69:Ā “Hong Kong Flu,” a global pandemic, began in Hong Kong and ultimately claimed 34,000 US lives.
This intense focus on SARS has opened a window of opportunity to pursue bilateral and international cooperation against infectious diseases.Ā The United States and WHO may be able to develop new institutional channels to foster long-term cooperation on health issues.Ā
Momentum is likely to flag if SARS continues to subside and political leaders lose interest.
Budget constraints and turf battles almost certainly will retard progress and agreements may fail to be implemented at the provincial, state and local levels if added responsibilities are not accompanied by additional funding.
Areas of Need.Ā Several countries already are seeking assistance from the WHO and the US CDC in an effort to strengthen their health systems.Ā Some even are moving to commit more resources.
Both China and Taiwan have held technical discussions with US officials exploring ways to improve their health system, and Beijing publicly has committed $1.3 billion in new funds.
Surveillance.Ā Despite substantial progress in recent decades in building networks to monitor disease, the surveillance systems in most countries remain weak.Ā Many surveillance systems have been built over the years to detect specific diseases, such as polio and guinea worm.Ā The WHO also has created a global network of over 100 centers in 83 countries to track influenza.Ā The longer-term challenge is to build networks throughout countries and regions and the means to issue warnings to national and international authorities.Ā
Systems focusing on specific diseases generally have been more cost effective than trying to increase surveillance for all diseases, but either approach leaves holes.Ā
International surveillance networks also must work out differences between countries over what health patterns are “normal” and which should set off alarm bells.Ā The death of working-age pneumonia patients in the United States would be so unusual it would trigger closer examination, but this phenomenon probably was not considered abnormal in China in the early stage of SARS.
Even if local health workers identify worrisome developments, many medical facilities in developing countries lack communications equipment and vehicles to alert national officials and transport samples or patients.
Although rapid on-line journal publication aided in sharing information on the new SARS virus, outbreak responders need to share date even earlier.
Health Surveillance and Biological Weapons
The SARS outbreak illustrates the difficulty in distinguishing the emergence of new infectious disease from the release of a BW agent.Ā Ongoing efforts to improve global health surveillance, however, probably will aid international monitoring for detecting the possible release of biological warfare agents, especially traditional types.Ā As baselines for natural diseases are established in the coming years, a deliberate release of traditional BW agents could be more readily recognized.Ā Unfortunately, many developing countries probably will not acquire domestic detection capabilities, such as tools to identify genetic sequences in disease organisms.Ā Moreover, history suggests that some countries will not support internal disease surveillance efforts for political or economic reasons, leaving significant gaps in a global surveillance system.
Epidemiological Expertise.Ā Many countries lacked trained experts to map the trajectory of SARS.Ā Such expertise was critical to understanding the transmissibility, lethality, and scope of the disease.Ā
Press reports indicate that Chinese officials have had trouble processing and sharing research information within China and with outsiders, such as WHO.
Laboratory Facilities.Ā Few countries have the sophisticated laboratories or trained personnel to do the hard science of cracking mysterious new illnesses.Ā As a result, regional or mobile labs may be the most viable prospect for speeding up diagnoses and research.
WHO reports that staff in over 90 percent of developing country laboratories are not familiar with quality assurance principles, and 60 percent of the lab equipment is inoperable or outdated.
Equipment.Ā The cost of basic diagnostic and protective equipment is relatively modest yet still unaffordable for many countries.Ā SARS highlighted a widespread shortage of ventilators to support patients with pneumonia.Ā The lack of adequate sterilization equipment raises the risk of spreading disease when medical instruments are reused.
The highest priority for many countries is likely to be diagnostic tests to determine which patients need to be isolated; the need for such tests would be all the more pressing if research indicates SARS can be transmitted through the blood supply.
Many countries need more ventilators to support patients with pneumonia.Ā In addition, negative pressure rooms to isolate infected patients are in shorter supply; even many hospitals in affluent countries are not likely to have enough rooms to handle a serious outbreak.
SARS and HIV/AIDS
SARS has focused greater international attention on the importance of health, but the new disease probably will not lead to a significant boost in the fight against HIV/AIDS in the coming years.Ā Indeed, many countries are likely to view spending on diseases like SARS and HIV/AIDS as a zero-sum game in the short term.
SARS is generating international interest in improving health surveillance systems that could broaden screening for HIV/AIDS as well, but the interests will not always coincide on allocating limited resources.Ā The small number of HIV/AIDS surveillance sites already in most countries is designed to gather health data on specific groups, such as young women, drug users, or prostitutes, rather than samples of the population at large.
Some countries may be willing to devote more resources to improving general health and fighting HIV/AIDS within their security services.Ā With HIV/AIDS prevalence rates running as high as 50 percent in some African militaries, a growing number of governments are working with the US on control programs.Ā Political leaders may see it as critical and cost effective to work with outsiders for better healthcare for soldiers as well.
China’s new Health Minister has said she plans to focus on HIV/AIDS now that SARS has subsided, according to press reports.Ā Some AIDS activists and NGOs within China also have expressed hope that the government response to SARS will translate into more action on HIV/AIDS.
A resurgence of SARS this winter could delay activity on AIDS, and some AIDS activists in China fear the government might believe the stringent controls used to fight SARS should be used against HIV/AIDS as well.
Developing Countermeasures.Ā Progress in developing diagnostic tests, treatments, and vaccines would fundamentally improve prospects for combating SARS.Ā This will take time, however, and first-generation products often are not completely effective without further research and improvement.
Tracking down infected and exposed persons on airline flights also could be improved significantly if airlines retained electronic records of passenger lists.
Political Hurdles.Ā Almost all countries will express support for improving international healthcare capabilities, but negotiations are likely to be contentious, and many players will see this as an opportunity to win concessions or score points with Washington.Ā Some areas of possible contention are:
Money.Ā Many developing countries will say they cannot improve their surveillance systems and healthcare infrastructure without significant outside assistance, in the form of training, equipment, or grants.
“Rich” vs. “poor” Diseases.Ā Some developing countries may argue that they will work to improve surveillance for diseases like SARS if the United States and the international community do more to help them fight diseases which claim more lives in their countries, such as malaria and tuberculosis.
Multilateral channels.Ā European countries are likely to use the focus on health issues to renew pressure on the United States to work through multilateral organizations such as the Global Fund for AIDS, Tuberculosis, and Malaria.
Pharmaceutical Access.Ā Any forum to discuss international health cooperation almost certainly will include some criticism ofĀ US positions in the WTO on pharmaceutical sales.Ā Research to develop tests, treatments, and vaccines is underway, but drug companies will have little incentive to bring such products to market without public sector support ifĀ SARS appears to fade away.
WHO Authority.Ā Some countries probably will argue for strengthening the authority of the WHO to sanction states that do not share health data or bar outside health experts from visiting.Ā Other countries, such as China and Malaysia, are likely to resist any moves they see as infringing on sovereignty.Ā Taiwan almost certainly will continue trying to use health issues to win recognition from WHO and other multilateral organizations.
Footnotes:
1Ā Anecdotal evidence suggests that some people with SARS may not have classic respiratory symptoms, which makes detection more difficult.
2Ā Quarantine is the sequestering of those possibly exposed to an infection, while isolation is the sequestering of those individuals with known or suspected infection.